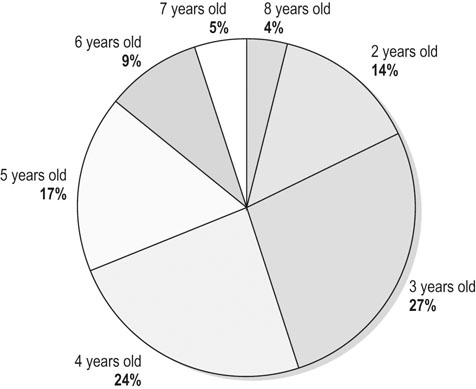
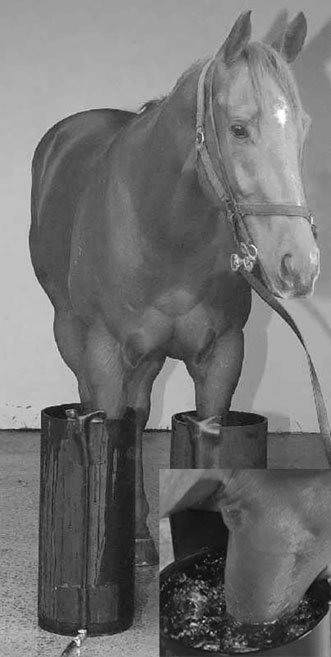
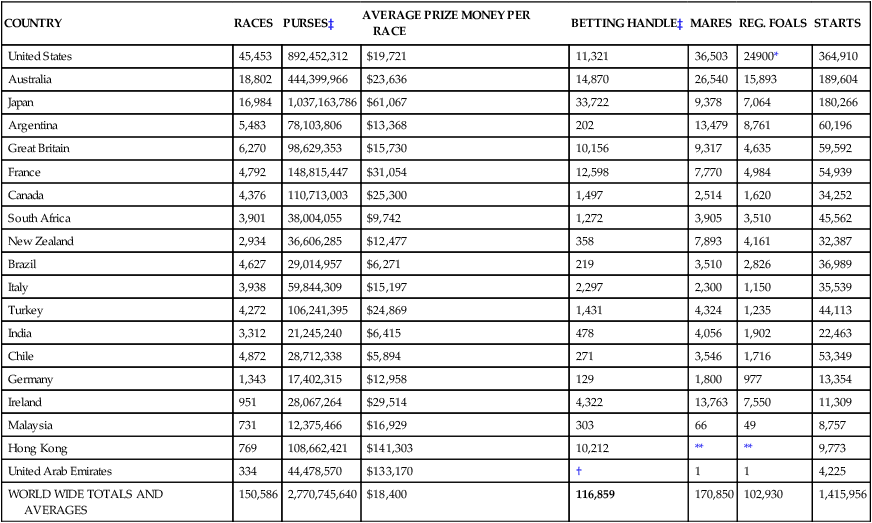
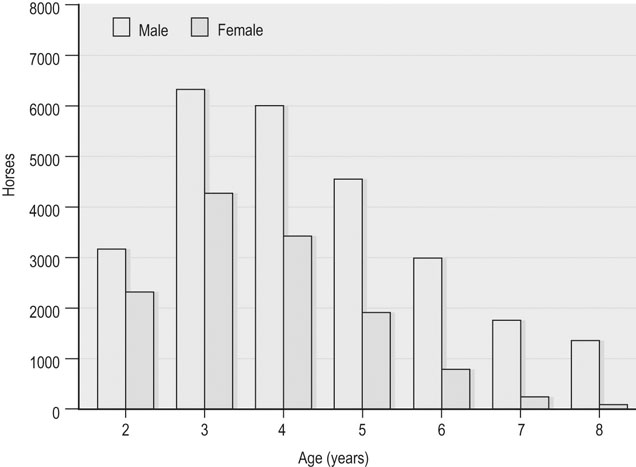
Thoroughbred racing evolved in England over 200 years ago and now exists in over 50 countries.1 A comparison of the size of Thoroughbred flat racing industries between some of the major racing countries based on foal crop, number of races and starters, prize money and betting turnover is illustrated in Table 48.1. Table 48.1 A comparison of some key industry figures for international Thoroughbred flat racing among major racing countries, for the year 2000 Betting handle figures are for the year 2011 IN USD$ MILLIONS Notes: US $ conversions of the Euro at 1.00 Euro = US $1.32 ***Not reported Source: International Federation of Horseracing Authorities 2011 annual report. Horses have their first opportunity to race as 2 year olds and their competitive longevity is the result of a multitude of veterinary and specific industry-based factors. Generally the majority of the racing population is made up of horses aged 2 through 5 years of age. Sex distribution of the racing population commences with relatively equal proportions of males and females as yearlings and 2 year olds.2,3 In subsequent racing years there is an attrition of females to breeding so that horses older than 4 years of age, are typically gelded males2–4 (Fig. 48.1 and Fig. 48.2). Age of first race start depends on athletic conformation, degree of maturity, genetics, aspirations and expectations of the owner and trainer, as well as race programming and prize money structure of the specific country. Attempts to judge musculoskeletal maturity and suitability for racing based on objective means such as physeal closure have been generally unsuccessful.5 The actual time of first race start is then dependent on the response to training, health, and soundness. Interestingly, in a study examining factors affecting early career wastage there was no correlation between sex and foaling date with time of first race start.3 While concerns over racing 2-year-old horses exist, two studies found that horses who raced first as 2 year olds had greater numbers of career starts and raced longer than did horses that commenced racing at an older age.2,3 This may in part be due to injury or disease that prevented these older horses competing as 2 year olds and which may have persisted further into their career. Wastage refers to all losses occurring at any stage in the breeding, growth, training and racing of a racehorse. Wastage includes all losses in breeding, deaths at any stage, lost training days, un-raced horses and retirement. Considerable wastage occurs in the Thoroughbred racing industry as a whole from the time that the mare is covered to the commencement of racing by the progeny. A UK-based wastage study calculated 72.8% of mares each year fail to have progeny that will go on to race between 2 and 4 years of age.6 In this study, the 1975 foal crop was followed and of those named and eligible for training only 50.6% raced as 2, 3, or 4 year olds; this result is confounded by horses reserved for National Hunt racing that did not race on the flat.6 A more recent UK study following 1022 foals found 52% entered training at 2 years of age. Similar prospective studies of 353 and 553 yearlings sold at auctions in Australia revealed that approximately 50% of these horses raced as 2 year olds and that 75 to 80% of horses had raced by their 6-year-old seasons.2,3 Lameness, followed by respiratory disease, is the major cause of wastage for Thoroughbreds in race training, manifesting as lost or affected training days.3,6–9 A UK wastage study found that 53% of horses showed lameness at some stage during a season and in 20% of cases the lameness was sufficient to prevent racing after injury.6 A subsequent study identified lameness (67.6%) and respiratory disorders (20.5%) as the most common cause of lost training days.7 Sore shins and inflammatory airway disease (IAD) were the most commonly encountered ailments in a UK study looking at failure to train and race.10 Similarly a US-based study looking at 95 horses over an 81-day period reported musculoskeletal injuries altering training or racing schedules in 35–55% of horses and preventing training or racing for a period of time in 26–46% of horses.11 A recent Australian wastage study of 2- and 3-year-old horses found that of lost or modified training days, 56% were due to lameness and 16% due to respiratory disease.12 Similar findings have recently been reported out of New Zealand, identifying musculoskeletal (82%) and respiratory diseases (11%) as the major cause of involuntary time out of training.9 A further reason horses may not race or race less than the average number of times is a ‘lack of athletic ability’.2,6 Breakdowns, fatal musculoskeletal injuries and sudden death during racing and training have been a focus of many recent studies, most aimed at identifying risk factors in an attempt to minimize these injuries.13–24 Regional differences exist with regard risk factors, prevalence and types of injuries between countries, states, regions and even individual tracks.14–18 The rate of breakdown injuries during racing differs between countries, with rates of 2.2/1000, 2.9/1000 and 21/1000 starters in the USA, Australia and Japan, respectively.13,14,19 These differences are difficult to interpret since they may in part be due to potential errors inherent with epidemiologic studies and different definitions of a breakdown.17–20 Approximate risk of fatal or catastrophic musculoskeletal injury are 0.6/1000 starters in Australia and 1.4–1.7/1000 starters in the USA, while in the United Kingdom there are 0.8 deaths/1000 starters.16,20–23 The reasons for differences in rates between countries are multifactorial, but dirt tracks, the presence of medications and longer races have all been implicated as possible factors factor contributing to a higher incidence of injury.23–26, An Equine Injury DatabaseTM was launched in 2008 with reported rates of fatality rates for 2008–2010 of 2.04–2.00/1000 starters.27 Catastrophic life-threatening injuries appear more likely to occur when racing, whereas non-fatal injuries are more common in training, which may be a function of speed.17,19 Breakdown injuries more commonly involve a forelimb than hindlimb, common sites of injury include fetlock and suspensory ligament, carpus, humerus, pelvis, tibia and superficial flexor tendon.14,19,20,22 There is evidence that pre-existing lesions predispose to catastrophic injuries, highlighting the value of early identification of such lesions in preventing injury.18,19,27–30 A multitude of risk factors contributing to breakdown injuries have been identified, including track characteristics,16,24,31 weather and season,24 race distance, starting position and race quality.20,32 Individual horse characteristics identified include racing frequency, training intensity, age at first start, duration of career, number of life time starts and the hoof or shoeing characteristics.15,16,24,33,34 Causes of sudden death other than fatal musculoskeletal injuries that have been described include ruptured aorta, myocarditis, valvular insufficiency, sclerosis of the coronary arteries, severe pulmonary hemorrhage and disseminated massive hemorrhage.35 Dorsal third metacarpal disease, carpal and fetlock joint disease and tendon or ligamentous injuries are the most common musculoskeletal problems leading to wastage.7,12,23 Routine, diligent observation of subtle changes in symmetry and meticulous palpation combined with use of hoof testers and flexion tests aids early identification of the most likely site of lameness. Where possible, targeted diagnostic anesthesia and imaging is used which is both economical and time saving. Quality imaging modalities including radiography, ultrasonography and scintigraphy, are essential for accurate diagnosis, treatment and prognostication. The presence of a secondary lameness is common and may go undetected without appropriate diagnostic anesthesia. Bilateral disease is commonly identified, particularly with carpal and fetlock injuries, tibial stress fractures and sites of osteochondrosis.36–41 Lameness examinations can be aided in the fractious patient with a small dose of sedation.42 Jogging in a circle or figure eight can also be useful for assessment of mild lameness and may help differentiate among sites of lesions causing lameness. Musculoskeletal diseases often require modifications to the training program, dictated by the disease or injury and the horse’s level of fitness. Changing the typical training formula is achieved by alteration of distance and/or speed. Terminology differs geographically in describing the approximate speeds horses train and race and understanding local terminology allows assessment of the current work load and appropriate suggestions with regard to modifications. Speed and distance may be expressed in furlongs (220 yards or approximately 201 meters) (Table 48.2). Table 48.2 Common terminology and speeds associated with Thoroughbred flat work. A furlong is a measure of distance used in horse racing (1/8th mile, 220 yards approx. 200 m) Trainers may have a variety of track surfaces available for training horses and advice with respect to training surface should be formulated based on knowledge of the local track characteristics, current track conditions and their contributions to injury risk. Traditionally turf has been associated with a lower risk of musculoskeletal injury than dirt, although confounding factors, primarily geographic, may contribute to this apparent lower risk.16,24,43 Some specific injuries appear to have an association with particular track surfaces. There is an apparent increase in the incidence of proximal suspensory desmitis in horses working on deeper surfaces with wood chip, dirt and synthetic tracks having an increased incidence over turf. (PE Sykes 2002 pers comm). The incidence of dorsal third metacarpal disease is higher in horses training on dirt compared to wood fiber tracks.44 Track condition or rating, has been implicated to influence the risk of injury;16,45,46 however, several large epidemiologic studies have found no association between track condition and injury rate.20,24 The mechanical characteristics of dirt and turf tracks are determined in part by their structure, with moisture content being the major variable influenced by weather and track maintenence.31,45,47,48 Injury risk is higher on turf tracks when the surface moisture content is low, resulting in a harder track and faster race times.16,19 Dirt tracks, on the other hand, have been associated with injuries under a variety of conditions, typically when moisture content is either too low or high or surface is of inadequate depth or composition.17,31,46 The mechanical characteristics of synthetic tracks, the majority of which have a wax component, are temperature dependent as well.49 Synthetic tracks appear to potentially decrease the risks of fatal musculoskeletal injuries; however, they may contribute to an increased risk of other non-fatal injuries. The major contributor to track performance and safety is likely to be associated with good track maintenance regardless of the surface. Unleveled track surfaces and areas where track is compacted such as ‘crossings’ for horse and vehicular access and areas around starting chutes have been associated with increased risk of injury.31,50 An inadequate banking or camber on turns may also contribute to injuries and alteration to track camber and surfaces have shown benefits in reducing injury rates in Thoroughbred and Standardbred racing.51–53 Therefore considerations to track characteristics should be given, especially with advice regarding horses working at high speed or rehabilitating from injury. Hill or incline work, either under saddle or on an inclined treadmill, allows work rate to increase while limiting speed.54,55 Inclines modify the activity and loads on various muscles,56 likely increasing the overall load on the hindlimbs that may be beneficial if attempting to strengthen the hind quarters, or being contraindicated in horses with hindlimb injuries. Walking in waist deep water in a pool or on a submerged treadmill provides greater work to the advancing limb and may benefit attempts to improve extensor and particularly quadriceps strength. Direction around turns (clockwise vs counterclockwise) influences limb-loading patterns with the lead limb subject to a greater load than the contralateral limb and this additional loading may predispose the lead limb to injury.20,57 Typically in a counterclockwise racing direction the horse preferentially leads with the left forelimb on the turn, and for clockwise racing the right forelimb with most horses changing to the opposite lead at some stage during the straight.58 Many injuries appear to have ‘lead’ or inside limb predilections dependent on the direction of racing such as dorsal third metacarpal disease,59,60 superficial digital flexor tendonitis,46 and antebrachiocarpal joint injuries, particularly the distal radius and proximal intermediate carpal bone.58 ‘Outside’ limb injuries are commonly associated with the medial middle carpal joint.58 Common musculoskeletal injuries associated with limb predilections may be minimized or prevented by training in both directions on turns. If introduced early in a training program it allows development of balance in both directions and minimizes repetitive loading of specified predilection sites. Walking exercise can be provided by either hand walking, mechanical walkers, or treadmills. Often overlooked, walking is useful in horses that are temporarily out of work and beneficial in horses susceptible to ‘tying-up’ or with chronic joint complaints. Walking after high-intensity exercise improves recovery.61 Ponying is useful for horses that do not settle at slow speeds or horses with back complaints, particularly wither or girth rubs. Some musculoskeletal back problems may be exacerbated, if the horse has tendency to track sideways.62 Swimming is a primarily aerobic exercise medium useful in reducing the effects of weight-bearing work and has been suggested to decrease the rate of musculoskeletal disease63 (Fig. 48.3). While allowing non-weight-bearing joint motion, swimming does not stimulate appropriate bone responses or maintain joint ligament tone.64 Potential complications of pools include infection of pre-existing wounds, interference injuries (higher risk in circular pools), exercise-induced pulmonary hemorrhage, colic and rarely drowning.65 Swimming increases muscle activity in some selected muscle groups and therefore may be contraindicated in the presence of primary muscle injuries.66 The effect of complete cessation of exercise on a horse’s level of cardiovascular fitness often depends on the horse’s stage of training. Horses early in their training phase appear to lose significant amounts of aerobic fitness within 2 weeks, whereas horses more advanced in training are slower to detrain, losing fitness over 4–6 weeks.67–69 Support bandaging can be useful to minimize swelling and edema associated with acute pathology or intermittent limb edema. The effectiveness of lower limb athletic support bandages or boots in preventing injury and their effect on performance is unknown; studies in healthy human athletes indicate they can be performance impairing.70 Studies of lower limb bandaging and athletic taping have had variable results in different studies: some have demonstrated a beneficial role through either reduced hyperflexion of the fetlock or reduced peak vertical forces,71–73 while other studies have failed to demonstrate benefits of taping or bandages.74 Support boots have been shown to reduce maximal extension of the fetlock at the walk and trot and may be beneficial reducing strain in the SDFT and suspensory ligament during rehabilitation.74,75 Improperly applied bandages may contribute to pathology and any bandaging may be contraindicated at high speed due to effects on heat dissipation.76,77 Work boots or padded bandages can be used to limit and reduce the severity of interference injuries. Cold therapy provides anti-inflammatory, analgesic effects and reduces cellular metabolic demands and should be considered in any acute or chronic injury.78 Rapid icing of acute injuries is followed by intermittent icing for approximately 48–72 hours until inflammation is resolved; chronic injuries benefit from icing after every bout of high-intensity exercise.55 Ice water slurries in large rubber boots are easy to apply, have the ability to include the carpus, and cool the limb more efficiently compared with commercial cold packs, reaching stable tissue temperatures in 10 minutes79 (Fig. 48.4). Excessive icing can cause dermatitis and ice burns. Limiting ‘icing’ times to less than 30 minutes, applying multiple applications with durations of at least 20 minutes out of the ice and application of a barrier layer (Cling Wrap, UK; Saran Wrap, USA; Glad Wrap, Australia) seems to minimize this complication. Early and aggressive anti-inflammatory therapy is indicated with all joint injuries provided the diagnostic process is not compromised. Once the level of joint compromise is determined, appropriate specific treatment can be pursued. Joint inflammation can be controlled with systemic non-steroidal anti-inflammatories (NSAIDs) at recommended doses for 24–48 hours, combined with cold therapy and bandaging. Cessation of high-intensity exercise and the substitution of walking is indicated while the joint is acutely inflamed. Trotting and swimming can be used to maintain activity until the horse is able to return to its previous level of work intensity. Rapid resolution of synovitis and capsulitis is beneficial in avoiding capsular edema and capsular fibrosis that may lead to reduced range of joint motion.80,81 Passive joint flexion may aid in maintaining range of joint motion. Intra-articular medications (as discussed in chapter 23) are likely to be most efficacious if used in a planned manner with consideration given to the horses training and racing schedules. Maximal anti-inflammatory effect is likely to be gained by early treatment followed by cessation of high-intensity exercise. Joints that are chronically affected should be treated after exercise on a day of planned high-intensity fast work, allowing at least 3–5 days or longer of modified low-impact activity prior to racing. Medicating chronically inflamed joints prior to prolonged layoffs may be beneficial in assisting the resolution of synovitis and capsulitis. The majority of veterinarians use corticosteroids alone or in combination with hyaluronic acid as the mainstay and first choice intra-articular therapy in Thoroughbred racehorses.82 Autologous conditioned serum is gaining popularity as a treatment, particularly in cases that either respond poorly to corticosteroid treatment or have a more chronic process requiring more regular and prolonged courses of therapy.82–84 Aseptic technique during intra-articular injections is essential and excessive ice therapy or the use of liniments or blisters should be avoided because the resultant dermatitis may compromise a suitable injection site (Fig. 48.5). Intermittent systemic anti-inflammatory therapy can be used in combination with long-term administration of disease-modifying osteoarthritic agents such as polysulfated glycosaminoglycans (PSGAGs), pentosan polysulfate, glucosamine and chondroitin sulfate. Stress-related cortical bone injuries ‘incomplete stress fractures’ have been reported in a variety of bones including the third metacarpal bone, tibia, humerus, pelvis, sacrum, lumbar vertebrae and scapula. These manifestations of bone fatigue have been postulated in some instances as precursors to complete spontaneous fractures.28,36,40,85–90 Similarly, exercise-induced subchondral bone injuries have been well documented in the third carpal bone and distal third metacarpal and metatarsal bones as well as other sites of osteochondral fractures, and have been proposed to be associated with cyclic loading and bone adaptation responses.89,91,92 Training protocols appear to directly influence bone-related injuries and disease. Changes in training intensity induce bone adaptation via altered forces and fatigue damage, with initial bone weakening due to increased bone porosity.93 The decreased mineral content is thought to significantly impact bone strength around 3 weeks after an alteration in training.94,95 and may take up to 3–4 months or longer to replace the lost bone, during which time the bone is weaker.94–96 It is the bone adaptation process itself that appears the more important component of bone weakening, rather than the fatigue damage.97 Two-year-old horses appear to be at greatest risk of adaptive bone pathology as their skeleton models and remodels in response to race training. The lowest bone mineral density in these horses occurs at 2–3 months after entering race training.96,98 Significant decreases in bone mineral content detrimental to bone strength occur during periods of inactivity,99 and are likely a result of a decrease in bone strains leading to extensive bone remodeling and increased porosity.93 A greater risk of bone fatigue-related injuries has been associated with return to work after periods of inactivity or lay-up.90,100 Since horses training at a slow speeds adapt their bones to that particular speed, the introduction of higher-speed pace work (‘breezing’) results in altered loads and bending forces requiring a further bone adaptation response, making bone susceptible to fatigue injury during this adaptation period.93,101 A study examining gait and speed as risk factors for fatigue injury of the third metacarpal bone in 2-year-old Thoroughbred racehorses recommended training modifications to reduce the incidence of ‘bucked shins’ consisting of reducing the extent of the low-speed long-distance work and increasing the frequency of the short-interval high-speed work.102 Therefore, allocating less training time to long-distance slow exercise and the introduction of earlier more frequent short distance fast exercise affords bone more time to adapt to race speeds.90 Problems that may be encountered include the inability to control young poorly educated horses, and the uninvestigated effects of this training protocol on other structures, particularly tendons and ligaments. The most appropriate training regimens to obtain optimal remodeling and modeling responses of bone that will best accommodate forces associated with racing and training are yet to be determined.103 Dorsal metacarpal disease manifesting as ‘bucked or sore shins’ is one of the most common causes of lost training days in 2-year-old Thoroughbreds; one survey reported it to affect 70% of Thoroughbreds, with increased risk of third metacarpal stress fracture within 6–12 months.93,104,105 Deciding if affected horses can continue training will depend on severity of the condition as determined by regular palpation of shins, lameness examination and radiographic evaluation. Early identification of disease through palpation and detection of subtle lameness allows early treatment and the majority of horses to remain in training. Treatment should include immediate modifications to the training program and aggressive anti-inflammatory therapy. Monitoring the horse’s gait during exercise and the level of pain on palpation of shins are useful in assessing the response to therapy. Swimming can be used to augment fitness, with the track regimen consisting of trotting and shorter distances of pace work regularly (for example, 1–2 furlongs every other day). Horses with more advanced dorsal metacarpal disease have marked pain, evidence of swelling or cortical lucency identified radiographically and should be removed from training on economic grounds for at least 6 weeks. They should be returned to training with suitable modifications to the training regimen as discussed above for horses with adaptive bone pathology. Recommended training schedules to avoid bucked shins and to manage horses with early evidence of bucked shins have been documented.106 Conservative management typically requires a minimum of 7 months rest with a variable degree of success in achieving healing.107,108 Surgery offers an advantage with both lag screw fixation or the combination of osteostixis and positional screw fixation are reported to be more reliable than osteostixis alone, with healing and screw removal at 2 months after surgery, followed by resumption of training within 1 month of screw removal.59,60,109 Stress fractures may be seen at a variety of sites (third metacarpal bone, tibia, humerus, pelvis, sacrum, lumbar vertebrae and scapula) and periods of reported rest for these fractures vary, so there is no clear consensus on an appropriate duration of stress fracture rehabilitation.110 Provided the stress fracture is not at risk of propagation to a complete fracture, general recommendations include stall rest with hand walking (the horse should be offered about 10 minutes hand walking twice daily, doubling weekly) until the horse is sound at the trot in a straight line. The horse should be evaluated for lameness after 2–4 weeks, first at the walk and if appropriate at the trot. Once sound at the trot, access to a small yard (20 feet square) for a further month is followed by a month of pasture release prior to return to training. A more rapid rehabilitation plan can be instituted under direct veterinary supervision with gradual introduction to low-level trot work after the month of stall rest and walking; however, such a program requires regular lameness and radiographic evaluation to monitor healing and possibly follow-up scintigraphic evaluation. This protocol can minimize time of maximal exercise restriction, but return to high-speed training should be delayed for at least 3 months from time of stress fracture diagnosis. Stress reactions and non-adaptive exercise-induced bone remodeling can also be managed with a similar approach. Subchondral bone injury and associated osteoarthritis occurs primarily in the carpus associated with the third carpal bone and the fetlock joint in the palmar/plantar metacarpal/metatarsal condyles and proximal sesamoid bones.85,89,111 The pathogenesis of these injuries is poorly understood but involves disease of both the articular cartilage and subchondral bone.91,92,111 Subchondral epiphyseal bone changes have been identified as potential precursor to some slab fractures of third carpal bone and condylar fractures of the cannon bone.85,89,112 The diagnosis and management of subchondral bone diseases is problematic and both joint and bone disease issues should be addressed. Often radiographic findings are equivocal and in these cases scintigraphy can be a useful aid in diagnosis. Determining the degree of subchondral bone injury and collapse on radiographs alone can be difficult; computed tomography and MRI are superior to radiographs in detecting subchondral bone pathology.113 Typically if subchondral bone damage is evident, prolonged periods of rest are usually required and surgery may be indicated particularly if disease is involving the carpus. Many advanced subchondral bone injuries carry a guarded prognosis for future athletic performance, due to chronic lameness. Major breakdown injuries in racing Thoroughbreds include severe bone and ligament injuries involving the fetlock (traumatic disruption of suspensory apparatus, condylar fractures and P1 fractures) and carpus (distal or proximal row slab fractures with unstable or collapsed carpus) as well as major fractures of the humerus, tibia and pelvis. Appropriate assessment and use of coaptation for transport of major musculoskeletal injuries has been well described elsewhere and is important knowledge for any racetrack veterinarian.114 Appropriate first-aid measures prevent further osseous and cartilage injury; maintain skin cover and prevent further damage to blood supply that may ultimately determine the ability to salvage the animal. Removal of these patients from the racetrack environment allows appropriate diagnostics, communications and decision making to take place. The combination of training and aging may have a progressive detrimental effect on tendon strength. Micro-trauma due to accumulated submaximal strains results in alterations in tendon structure that decrease its ability to cope with cyclic strains and may ultimately result in injury.115,116
Veterinary aspects of training Thoroughbred racehorses
Demographics and wastage
COUNTRY
RACES
PURSES‡
AVERAGE PRIZE MONEY PER RACE
BETTING HANDLE‡
MARES
REG. FOALS
STARTS
United States
45,453
892,452,312
$19,721
11,321
36,503
24900*
364,910
Australia
18,802
444,399,966
$23,636
14,870
26,540
15,893
189,604
Japan
16,984
1,037,163,786
$61,067
33,722
9,378
7,064
180,266
Argentina
5,483
78,103,806
$13,368
202
13,479
8,761
60,196
Great Britain
6,270
98,629,353
$15,730
10,156
9,317
4,635
59,592
France
4,792
148,815,447
$31,054
12,598
7,770
4,984
54,939
Canada
4,376
110,713,003
$25,300
1,497
2,514
1,620
34,252
South Africa
3,901
38,004,055
$9,742
1,272
3,905
3,510
45,562
New Zealand
2,934
36,606,285
$12,477
358
7,893
4,161
32,387
Brazil
4,627
29,014,957
$6,271
219
3,510
2,826
36,989
Italy
3,938
59,844,309
$15,197
2,297
2,300
1,150
35,539
Turkey
4,272
106,241,395
$24,869
1,431
4,324
1,235
44,113
India
3,312
21,245,240
$6,415
478
4,056
1,902
22,463
Chile
4,872
28,712,338
$5,894
271
3,546
1,716
53,349
Germany
1,343
17,402,315
$12,958
129
1,800
977
13,354
Ireland
951
28,067,264
$29,514
4,322
13,763
7,550
11,309
Malaysia
731
12,375,466
$16,929
303
66
49
8,757
Hong Kong
769
108,662,421
$141,303
10,212
**
**
9,773
United Arab Emirates
334
44,478,570
$133,170
†
1
1
4,225
WORLD WIDE TOTALS AND AVERAGES
150,586
2,770,745,640
$18,400
116,859
170,850
102,930
1,415,956
Musculoskeletal diseases
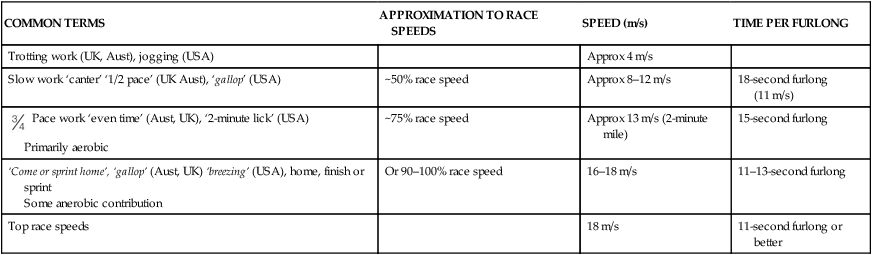
Exercise modification
COMMON TERMS
APPROXIMATION TO RACE SPEEDS
SPEED (m/s)
TIME PER FURLONG
Trotting work (UK, Aust), jogging (USA)
Approx 4 m/s
Slow work ‘canter’ ‘1/2 pace’ (UK Aust), ‘gallop’ (USA)
~50% race speed
Approx 8–12 m/s
18-second furlong (11 m/s)
 Pace work ‘even time’ (Aust, UK), ‘2-minute lick’ (USA)
Pace work ‘even time’ (Aust, UK), ‘2-minute lick’ (USA)
Primarily aerobic
~75% race speed
Approx 13 m/s (2-minute mile)
15-second furlong
‘Come or sprint home’, ‘gallop’ (Aust, UK) ‘breezing’ (USA), home, finish or sprint
Some anerobic contribution
Or 90–100% race speed
16–18 m/s
11–13-second furlong
Top race speeds
18 m/s
11-second furlong or better
Bandages and bandaging
Cold therapy
Joint diseases and injuries
Medical management of joint injuries and disease

Bone-related injuries and diseases
Training modifications
Dorsal metacarpal disease
Third metacarpal dorsal cortical stress fractures
Stress fractures at other sites
Subchondral bone injuries
Breakdown Injury
Tendon- and ligament-related injuries and diseases
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Veterinary aspects of training Thoroughbred racehorses