CHAPTER 21 The Spleen
The spleen is part of the hemolymphatic system and consists of a cellular parenchyma of red and white pulp supported by a stroma of reticular fibers. It is surrounded by a connective tissue capsule containing variable amounts of smooth muscle. As a component of the hemolymphatic system, the spleen serves several purposes. In addition to an important role in the immune response, its functions include storage of platelets and mature red blood cells (RBCs); maturation of reticulocytes; phagocytosis and destruction of RBCs, platelets, white blood cells (WBCs), and foreign particles; and extramedullary hematopoiesis.1 The nature of these functions causes the gross and microscopic appearance of the spleen to be affected by a variety of systemic inflammatory diseases and hematologic disorders. As with other organs, the spleen is subject to cell growth disturbances (e.g., hyperplasia, atrophy), circulatory abnormalities (e.g., hematoma, congestion, thrombosis, infarction), inflammation, and neoplasia (primary and metastatic).2 Several of these processes, either alone or in combination, may result in splenic enlargement.
Splenomegaly is a common clinical abnormality in small animal practice and is usually detected by palpation or imaging techniques. Minor degrees of splenomegaly can be revealed radiographically or ultrasonographically. Depending on the cause, splenomegaly may be accompanied by hematologic abnormalities, such as hemolytic anemia, thrombocytopenia, leukopenia, leukemia, or hemolymphatic neoplasia.3 A complete blood count and careful examination of RBCs, WBCs, and platelet morphology on a peripheral blood film are indicated. Causes of splenomegaly in dogs and cats are listed in Table 21-1.2–4
Table 21-1 Causes and Characteristics of Splenomegaly in Dogs and Cats4
| Cause | Type of Enlargement | Severity of Enlargement |
|---|---|---|
| Hyperplasia | Symmetric | Mild to moderate |
| Infection | ||
| Immunologic disease | ||
| Extramedullary Hematopoiesis | Symmetric or nodular | Mild to moderate |
| Hemolymphatic Neoplasia | Symmetric | Moderate to severe |
| Lymphoproliferative neoplasms | ||
| Myeloproliferative disorders | ||
| Systemic mastocytosis | ||
| Malignant histiocytosis | ||
| Splenic Neoplasia | Asymmetric or nodular | Mild to severe |
| Hemangioma/hemangiosarcoma | ||
| Fibrosarcoma | ||
| Leiomyosarcoma | ||
| Metastatic neoplasms | ||
| Circulatory Disturbances | ||
| Hematoma | Asymmetric | Mild to moderate |
| Portal hypertension | Symmetric | Mild to moderate |
| Torsion | Symmetric | Severe |
Once splenomegaly is detected, the specific cause should be determined, because splenic enlargement is usually a secondary manifestation of some other clinical problem. A complete physical examination and assessment of historic information are essential. Careful palpation and radiographic studies should reveal the severity of splenomegaly and whether the enlargement is diffuse and symmetric or localized to one area of the spleen (i.e., asymmetric). Ultrasonographic examination can be more sensitive and provides a more detailed assessment of architectural abnormalities in the spleen. By visualizing small nodules, target lesions, or changes in echogenicity in the spleen, ultrasound examination frequently reveals suspect areas of neoplasia, hyperplasia, inflammation, or extramedullary hematopoiesis that would not be visible radiographically. Indications for splenic aspiration are summarized in Box 21-1.5
Box 21-1 Indications for Cytologic Examination of the Spleen5
COLLECTION OF SPLENIC SPECIMENS
Fine-Needle Aspiration
Aspiration of splenic samples through the abdominal walls of live animals should be carefully considered. An enlarged spleen can be turgid, friable, and engorged with blood. Profuse intraabdominal hemorrhage and tumor metastasis within the abdominal cavity are possible complications of this procedure; aspiration of the spleen should be considered carefully when hemangiosarcoma is suspected.3,6 Recent studies in dogs and people concluded that thrombocytopenia, number of needle passes during collection, repeat aspirations, and core biopsies were not associated with an increase in the number or severity of complications.7,8 In live dogs and cats, aspiration of the spleen is indicated when the cause of splenomegaly cannot be determined by other means. The technique is especially useful in detecting splenic enlargement caused by hemolymphatic neoplasia and has some value in splenomegaly caused by infectious, immunologic, or hemolytic disease (see Table 21-1).
The spleen is gently pressed against the abdominal wall at the prepared site. The needle with attached syringe is inserted through the skin and muscle layer into the spleen. Withdrawing the syringe plunger produces negative pressure while the needle is moved within the spleen along several axes. Maintaining suction while redirecting the needle in the parenchyma collects cells and tissue fragments from several areas. Negative pressure on the plunger should be released when a small amount of bloody fluid appears in the syringe tip. Excessive hemorrhage and dilution of the sample with blood should be avoided. It is very important to release the syringe plunger before the needle is withdrawn from the spleen. Immediately after withdrawing the needle from the animal, small drops of the aspirate are applied to glass slides. The consistency of the aspirated specimen determines the method of smear preparation.9 Most splenic aspirates have the consistency of blood, and slides are prepared in the same manner as blood films. Specimens that are thick or contain tissue fragments are prepared by the squash technique, with the material gently compressed between two slides. The cells are spread by pulling the slides across each other. Chapter 1 contains a detailed description of slide preparation techniques.
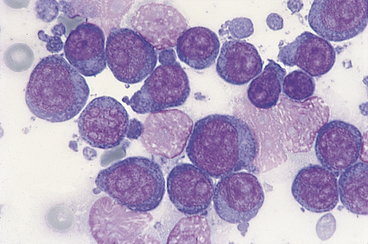
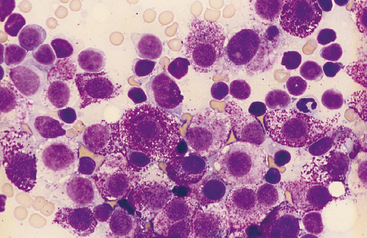
Impression smears of splenic tissue from surgical biopsies or necropsy specimens have several uses. In some situations, an immediate diagnosis may be obtained. For example, a homogeneous population of large lymphoblasts (Figure 21-1) or a pure population of mast cells (Figure 21-2) confirms a diagnosis of lymphoma and mastocytoma, respectively. In other cases, cytologic findings may eliminate neoplasia from the differential diagnoses and allow other causes of splenomegaly to immediately be pursued.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


