CHAPTER 26 Peripheral Blood Smears
Blood smear preparation is easy and inexpensive, and smear examination is readily learned with adequate background information and routine practice. This chapter describes techniques of preparation and interpretation of canine and feline blood smears and addresses integrating findings from blood smears with other parameters in CBCs. Supplementary information on interpreting routine hematologic parameter values is available in several well-written reviews and texts.1–5
HEMATOLOGIC REFERENCE RANGES
Hematologic reference ranges must be established by individual diagnostic laboratories; however, published reference ranges can be used as a general guide for in-clinic laboratories. Typical values for dogs and cats are listed in Table 26-1. Certain physiologic factors occasionally cause a healthy patient’s hematologic values to deviate from reference ranges. Because they are rapidly expanding their vascular space, very young animals tend to have relatively low hematocrits. Because they are also actively replacing fetal with adult red blood cells (RBCs), animals in early growth periods have greater RBC anisocytosis, polychromasia, and incidence of nucleated RBCs when compared with mature animals.
Relatively high lymphocyte counts are also common in young animals, and lymphopenia is suggested if lymphocyte counts drop below 2000 cells/μl in puppies and kittens under 6 months of age.3 Transient elevations above the reference range for lymphocyte counts are common in excited or vigorously exercised patients, especially if they are immature. This epinephrine-induced response can also result in temporarily increased counts of other WBC types in the peripheral blood of healthy patients. At least one canine breed, the Greyhound, has hematologic reference ranges reported to fall slightly outside of reference ranges commonly used for the species.6,7 Although these normal physiologic conditions should be considered, they generally explain less than 5% of the patient values that fall outside reference ranges for any single hematologic parameter.
SMEAR PREPARATION
Glass Slides
Smears are prepared on glass slides by placing a drop of blood (2 to 3 mm in diameter) on the broad face of the slide about 1.0 to 1.5 cm from the frosted border (or edge of a nonfrosted slide). Another clean, dry slide (i.e., spreader slide) is held loosely against the surface of the first slide at a 30-degree angle and drawn smoothly toward the blood drop, as illustrated in Figure 1-16. The spreader slide should be brought to a position where it just meets, but is not drawn into, the blood drop. When the spreader slide makes contact with the blood, capillary action immediately distributes the blood between the two slides. Then, with no downward pressure, the spreader slide is quickly and smoothly swept across the remaining length of the underlying slide.
Ideally, blood smears have a smooth transition from the thick region to the feathered edge and cover an area half the length and slightly less than the width of the slide (see Figure 1-16, D). If the edge is blunt instead of feathered, the second slide was probably raised off the first before the blood was spread completely. Unequal smear thickness usually results from the spreader slide being held at too obtuse an angle or placing too much pressure on the first slide while spreading the blood. Too much pressure on the second slide can also result in WBC clumping along the smear’s feathered edge. Too little pressure can result in short, thick smears. Smear thickness can also be affected by the viscosity of the blood sample. Adjusting the angle at which the second slide is held against the first can help compensate for very viscous (e.g., hemoconcentrated) or watery (i.e., anemic) blood samples. A more obtuse, 40- to 45-degree angle between the two slides makes thicker smears for very anemic samples, and an angle less than 30 degrees may be necessary for preparing smears of severely hemoconcentrated blood. Smears need to be thoroughly air-dried before staining; those that are thick may require additional drying time. Use (at the low setting) of a heat block or a blow dryer may shorten the drying time.
TROUBLESHOOTING
Artifacts of Cell Morphology and Staining
Crenated Erythrocytes
Crenated erythrocytes (see Figure 26-33), artifacts especially common in feline blood samples, have a thorn-apple shape with many short, uniformly spaced, blunt or pointed spicules that protrude from the cell membrane. Crenated RBCs can result from drying the smear too slowly or a relative excess of anticoagulant in the sample. Prolonged storage time of the blood (e.g., more than 2 hours at either 4° C or room temperature), particularly with an EDTA anticoagulant, can also result in RBC crenation. Differences in surface tension between the cell membrane and the glass slide may be an unpredictable cause of the artifact.
In Vitro Aging Artifacts
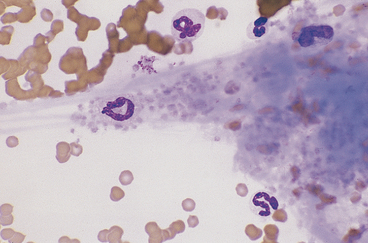
These are common in smears made from blood samples left at room temperature for more than 2 to 4 hours or refrigerated for longer than 12 hours. Neutrophils, monocytes, and immature and neoplastic WBCs degenerate slightly earlier than other cell types. The nuclei of affected cells initially become condensed and homogeneous-staining, and segmentation of granulocyte nuclei becomes more prominent, with only thin stands of chromatin separating lobules (e.g., hypersegmented neutrophils). Basophilia and vacuolation may be evident in the cytoplasm of neutrophils, and nuclei later become pyknotic and fragmented (Figure 26-1). The cytoplasmic borders of degenerating cells often show blebbing (Figure 26-2), and the cytoplasm of lymphocytes and monocytes may become vacuolated. These changes interfere with accurate identification of cell type and invalidate differential WBC counts if more than 10% of the cells in the smear are affected. Platelet aggregation/agglutination is also prevalent in aged samples. Avoiding aging artifacts is one reason to include fresh well-made smears with a sample submitted for hematology analysis to an outside laboratory.

Pale or Unstained Nuclei
Pale or unstained nuclei (Figure 26-3) on smears suggest that there has been inadequate staining time, or the stain has aged. Of the three-step quick stain solutions, the methylene blue mixture is usually that which has begun to degrade and may require longer incubation time with the smear or replacement. On Wright’s-stained preparations, pale nuclei with bright orange-red RBCs can result from overzealous washing or low pH of the buffer. Conversely, Wright’s-stained smears with pale nuclei and RBCs that stain slightly brown to green may occur when preparations are thick, inadequately washed, or stained with too little or too alkaline a buffer. A neutral buffer (i.e., pH 6.4 to 7.0) is most effective for Wright’s staining. The pH of the distilled or tap water wash solution can occasionally interfere with the intensity of the nuclear staining with both Wright’s and quick stains. Additional causes of inadequate nuclear staining are noted in Table 1-3.
Drying Artifact
Drying artifact (Figures 26-4 and 26-5) results if a smear is insufficiently air-dried before it is stained. The artifact is recognized in RBCs as round to crescent-shaped, punched-out regions or refractile vacuole-like structures. Stain condensations may border these pale cell areas or precipitate in the background between cells.
Stain Precipitate
Stain precipitate is more often a problem with Wright’s stains than with quick stains. Wright’s stain will precipitate in storage, if incubated on a slide too long, or if insufficiently washed from a slide after incubation. Precipitate formed during storage and from insufficient washing occurs as random aggregates of spherical and dumbbell-shaped granules that appear both in and out of the smear’s plane of focus (Figure 26-6). With prolonged incubation time, stain precipitate appears throughout the smear as uniformly dispersed, irregular globules of stain. Precipitate formed during storage can be removed by filtering the stain through Whatman filter paper into clean vials.
NORMAL CELL COMPONENTS OF BLOOD
White Blood Cells
Neutrophils
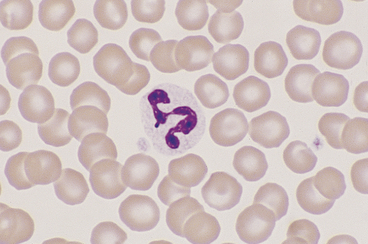
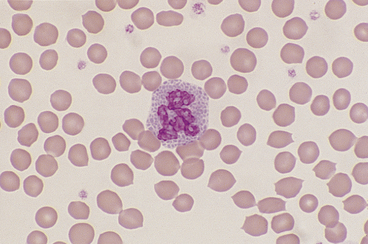
Canine and feline neutrophils have similar appearance on blood films (Figure 26-7). The neutrophil nucleus is elongate and separated into multiple lobules by invaginations of the nuclear border. Demarcations between lobules are seldom distinct enough to be considered filamentous. Chromatin is organized into dense clumps of dark purple to black staining heterochromatin separated by narrow areas of less condensed euchromatin. Cytoplasm is clear, pale eosinophilic to faintly basophilic with a fine grainy texture, and rarely, contains one or two small vacuoles. Neutrophil granules range from indiscernible to faintly eosinophilic but are pale and much smaller than the prominent granules of mature eosinophils.
Band Neutrophils
Band neutrophils, low numbers of which occur in the peripheral blood of healthy dogs and cats, have an elongate, U- or J-shaped to slightly twisted nucleus with less chromatin condensation than mature neutrophils (Figure 26-8). Nuclear lobulation is absent or poorly defined. Constrictions of canine band neutrophil nuclei are less than half the width of the remainder (nonconstricted sections) of the nucleus; feline band neutrophils lack nuclear constrictions entirely. Cytoplasm is similar in granule content and staining to that of mature neutrophils.

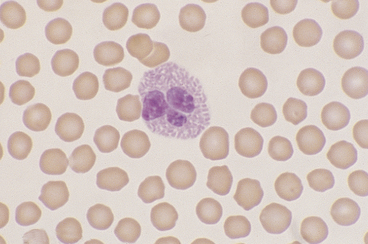
Monocytes
Canine and feline monocytes are larger than neutrophils and similar in size to eosinophils and basophils. Nuclei vary greatly in morphology, ranging from elongate U shapes that resemble band neutrophils to irregular multilobulated forms. The nuclear chromatin of monocytes is generally distinct from that of both mature and immature granulocytes and is characteristically lacy to ropy with only a few small isolated clumps of heterochromatin (Figure 26-9). The moderate to abundant gray-blue cytoplasm of monocytes has a ground-glass texture, is often sparsely dusted with minute eosinophilic granules, and occasionally contains vacuoles. Cytoplasmic borders are usually irregular, sometimes with fine, filamentous, pseudopodia-like extensions. Because of their relatively large size, monocytes may be concentrated along the feathered edge, and their proportion underestimated in blood smear differential WBC counts.

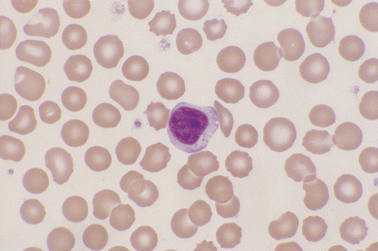
Lymphocytes
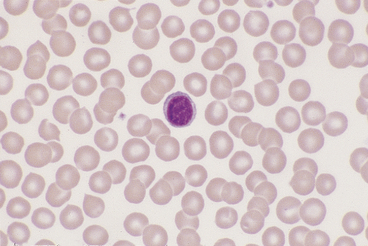
Lymphocytes vary in size in the peripheral blood of dogs and cats, with small cells predominating. Small lymphocytes have densely staining, round to oval nuclei that are sometimes slightly indented and usually have large, well-defined chromatin clumps (Figure 26-10). Alternatively, nuclear chromatin may appear smudged, especially when stained with a quick stain. The moderately blue cytoplasm of small lymphocytes is scant, and cytoplasmic borders are partially obscured by the nuclei, particularly with feline lymphocytes. Larger lymphocytes in peripheral blood have less densely staining, but still clearly clumped, nuclear chromatin. Cytoplasm of the larger cells is more abundant and ranges from light to moderately basophilic. Some lymphocytes have a few variably sized eosinophilic cytoplasmic granules that are usually concentrated within a single perinuclear cell area (Figure 26-11).
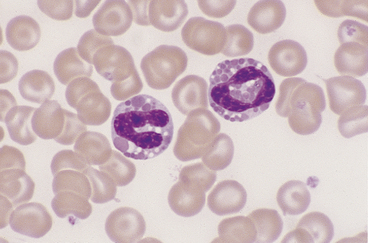
Eosinophils
Eosinophils, which are slightly larger than neutrophils, can usually be found in very low numbers on blood smears of healthy dogs and cats. Nuclei are less lobulated (often being divided into only two distinct lobules) with less condensed chromatin (Figure 26-12) than those of mature neutrohils. Cytoplasm is clear to faintly basophilic and contains prominent pink granules, which are abundant, small, and rod-shaped in cats (Figure 26-13) but vary widely in number and size in dogs. Canine eosinophils occasionally contain a single, large granule that may be mistaken for an inclusion body or unusual organism (Figure 26-14). Eosinophils of Greyhounds are peculiar in that they may appear vacuolated on smears—a breed difference that has been attributed to differential staining properties of the specific granules.8 Eosinophil granules that are ruptured in vitro are also sometimes freely scattered in the background of canine and feline blood smears.

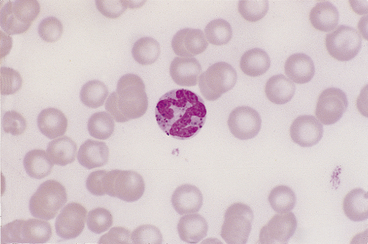
Basophils
Basophils are the largest of the mature granulocytic cell types and rare in peripheral blood of healthy dogs and cats. Nuclei are less densely staining and have fewer lobulations and a more elongated, ribbon-like appearance than the nuclei of other granulocytic cell types (Figure 26-15). Cytoplasm is moderately blue-gray to slightly purple and usually contains granules. In dogs, basophil granules are usually low in number and stain dark blue to metachromatic. Canine basophils also occasionally lack obvious granules but are recognizable by their size, nuclear morphology, and cytoplasmic staining (Figure 26-16). In cats, basophils contain abundant oval, pale lavender to gray specific granules (Figure 26-17), although immature basophils may also contain a few primary, dark purple granules.

Platelets
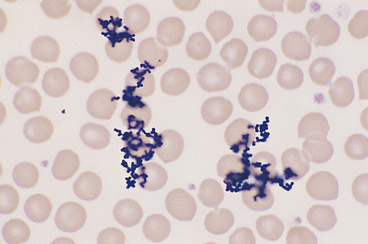
Canine and feline platelets appear oval, round, or rod-shaped on peripheral blood smears. Their clear to pale gray cytoplasm usually contains a central cluster of eosinophilic to metachromatic granules. Platelets normally vary in size from about one fourth to two thirds of the diameter of RBCs in canine blood, and occasionally are even larger than the RBCs in feline blood. Partially activated platelets have a spider-like appearance with thin cytoplasmic processes extending from a small spherical cell body. Platelets may also appear aggregated (Figure 26-18) or agglutinated into an amorphous mass on blood smears, a finding particularly common in feline blood smears. Aggregated and agglutinated platelets are usually pushed to the feathered edge, which may result in the false impression of thrombocytopenia if only the monolayer of the smear is evaluated.
ALTERATIONS OF RBCs IN DISEASE
Alterations in RBC Numbers
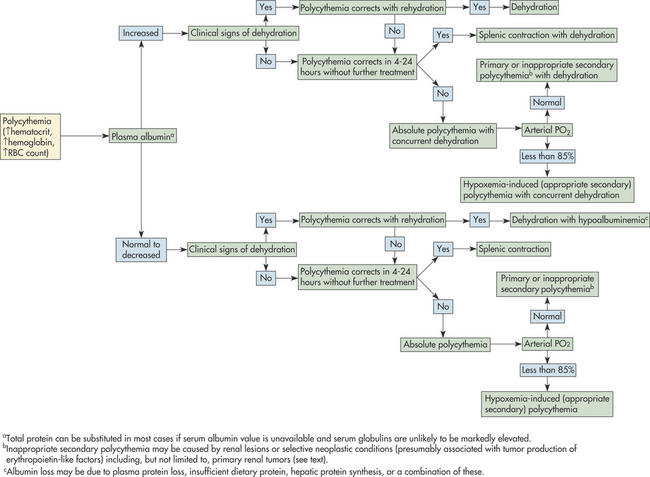
Absolute polycythemia secondary to inappropriate erythropoietin production, and primary polycythemia, or polycythemia vera, which is independent of erythropoietin levels, are both rare in dogs and cats. These two conditions are tentatively diagnosed by excluding the more common causes of erythrocytosis. Polycythemia associated with tumor erythropoietin production has been reported in dogs with renal and nonrenal tumor types, with the latter including cecal leiomyoma, nasal fibrosarcoma, and extradural schwannoma.9–11 Inappropriate administration of recombinant erythropoietin or androgens may also be a cause of absolute secondary polycythemia in dogs or cats as in other species, although treatment with human erythropoietin can also lead to red cell aplasia in both species.12 The algorithm of Figure 26-19 may further help in determining the cause of polycythemia in dogs and cats.
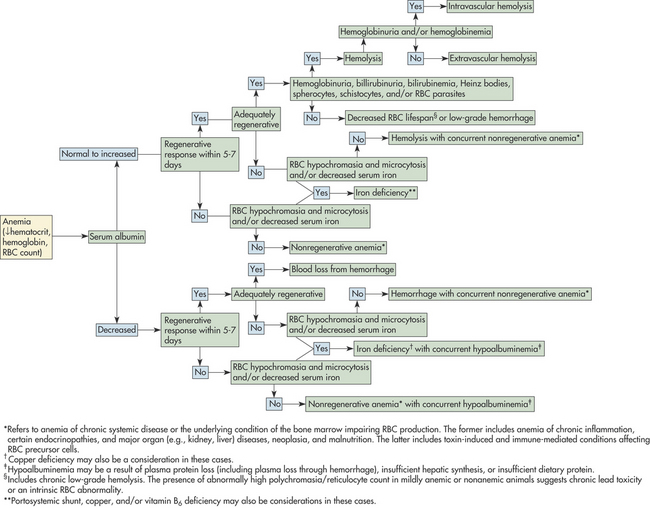
Anemia is an especially common finding in dogs and cats and can be secondary to almost any type of illness. Anemia is often suspected before blood samples are collected based on a patient’s clinical signs and physical examination. Evidence to support the condition as being acute or chronic can be derived from the clinical presentation and history. An animal with peracute to acute blood loss is often anxious and tachypneic and may have mucous membranes that are paler than expected for the degree of anemia as a result of transient peripheral vasoconstriction. With chronic blood loss, through upregulation of RBC 2,3-diphosphoglycerate in dogs and likely by an alternative mechanism in cats, oxygen is more readily released from hemoglobin to the tissues. Animals with chronic anemia are apt to be relatively inactive and show distress and dyspnea only if further stressed by physical exertion or an additional medical condition or if the blood loss is severe. A dog or cat presenting with a packed cell volume (PCV) of 12% or less typically has some degree of chronic anemia, because acute or subacute blood loss to this magnitude is generally not life-supporting. Blood smear examination, as described in the following section and Figure 26-20, may further aid in determining the cause of anemia in dogs and cats.
Blood Smear Examination in the Evaluation of Anemia
Cytologic examination of peripheral blood is important in determining the cause, treatment, and prognosis of a patient’s anemia. The procedure is also valuable in monitoring anemic conditions over time. Alterations of red cell morphology are usually most indicative of the primary cause of the anemia. For example, anisocytosis may be detected in animals with regenerative erythropoietic response or immune-mediated hemolysis with spherocytic RBC, and is especially profound when the two conditions are concurrent (see Figure 26-26). An increasing proportion of large, immature RBCs over time without a change in absolute red cell count suggests that an animal has persistent blood loss (or hemolysis) and a responsive marrow. Other components of the smear, including leukocytes and platelets, may also provide clues about the cause of anemia. Increased numbers of normal or enlarged platelets may been seen in association with acute or persistent blood loss. Low platelet numbers support platelet consumption or destruction, with anemia secondary to hemorrhage or immune-mediated hemolysis. Leukocytosis is usually also seen with immune-mediated red cell destruction, whereas leukopenia (especially neutropenia) and thrombocytopenia occur concomitant with anemia with impaired bone marrow hematopoiesis.
Reticulocyte Evaluation and Quantitation
Method
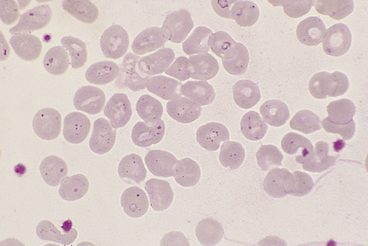
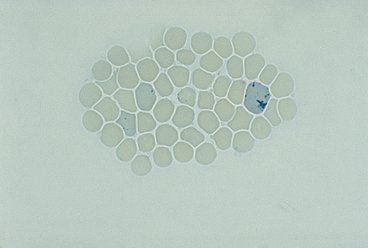
Canine reticulocytes are of the aggregate type, recognized by their dark blue, interlacing network of cytoplasmic precipitate. Feline reticulocytes are of two readily recognizable types, aggregate reticulocytes (as in dogs) and punctate reticulocytes (Figure 26-21). Punctate reticulocytes lack the reticular pattern of cytoplasmic staining but contain a few scattered, variably sized, dark blue cytoplasmic granules. These two reticulocyte types are counted separately in feline blood because their kinetics during a regenerative response differ. Note that epierythrocytic Hemobartonella felis organisms, basophilic stippling, and drying artifacts on RBCs can appear similar to and may need to be differentiated from punctate reticulocytes on NMB-stained feline blood smears.
Interpretation
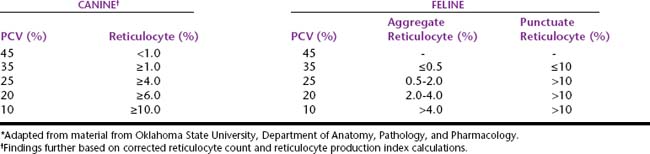
A maximal erythropoietic response from the bone marrow is expected within 7 days of the onset of anemia. At this time, a reticulocyte percentage that is at least equal to the average expected value for the species and the corresponding level of anemia (Table 26-2) represents an adequate marrow response, which is indicative of blood loss from hemorrhage or hemolysis. A reticulocyte count greater than 50% of the expected response but less than that considered adequate for the species and the severity of anemia represents an inadequately regenerative marrow response. Inadequately regenerative anemias occur in animals with hemorrhage or hemolysis concomitant with impaired marrow erythropoiesis. Animals whose marrow has had time to respond (about 7 days) but who have <50% of the expected reticulocyte response for their corresponding hematocrit should be considered to have a nonregenerative anemia. Note that erythropoietic responses are highly variable and less readily classified in dogs with only mild anemia (i.e., PCV >25%).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


