CHAPTER 13 The Musculoskeletal System
SAMPLE COLLECTION
Collection of material from bone lesions for cytologic examination can be complicated by the hardness of cortical bone. Lesions that have a major soft tissue component can be aspirated by techniques similar to those for any soft tissue mass (see Chapter 1). Even heavily mineralized masses can often be aspirated with a fine needle by careful palpation and exploration of the lesion surface. Examination of radiographs may reveal portions of the lesion that are less heavily mineralized and more likely to produce useful aspirates. Some lesions in which the cortical bone remains intact will not yield to fine-needle aspiration. In such instances, the best way to obtain diagnostic material is to use a trephine to obtain a core biopsy specimen. Imprints can be made for cytologic evaluation before the specimen is fixed in formalin for histologic processing. Remember it is important to keep cytology smears away from formalin fumes because these will inactivate cellular enzymes and interfere with cytologic staining and evaluation.
Cytologic specimens from skeletal muscle lesions can be collected by methods similar to those used for dermal and subcutaneous masses that are described in Chapter 5.
INFLAMMATORY DISEASES
Inflammatory lesions of the skeleton are important causes of disease in domestic animals, and cytology can be a valuable diagnostic tool in identifying certain lesions. Cytologic specimens from inflammatory lesions of bone are generally similar to exudates from other organs. Neutrophils typically predominate in specimens from animals with osteomyelitis, although activated macrophages and multinucleate giant cells are a significant component of some exudates. Inflammatory lesions that are accompanied by new bone proliferation may yield cytologic specimens that also contain small numbers of osteoblasts, which typically range from plump and ovoid to fusiform with round to ovoid eccentric nuclei and dark blue cytoplasm. They differ from neoplastic osteoblasts in that they are smaller and more uniform and lack nuclear manifestations of malignancy (see Chapter 2).
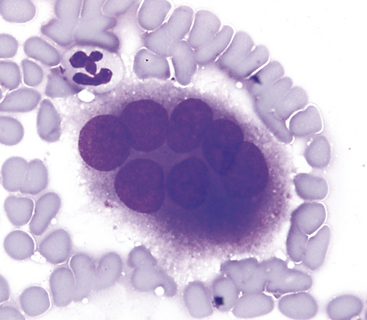
Osteoclasts may also be found in small numbers in specimens from inflammatory lesions. These cells resemble multinucleate giant cells and arise from precursor cells of the monocyte/macrophage cell line. They are very large and irregularly shaped with variable numbers (typically 6 to 10) of uniform, round nuclei arranged randomly throughout the cell and the abundant, light blue cytoplasm (Figure 13-1).
Some specific infectious agents that cause osteomyelitis may be identified in cytologic preparations. Actinomyces spp. occasionally cause osteomyelitis in dogs. These organisms appear as branching, filamentous rods that cannot be distinguished from Nocardia spp. on Romanowsky-type stains. Neutrophils predominate in aspirates from actinomycotic lesions as well as in aspirates from other types of bacterial osteomyelitis. Bacterial cocci in such aspirates are indicative of infection by staphylococci or streptococci, and bipolar rods are typical of infection by gram-negative organisms.1,2
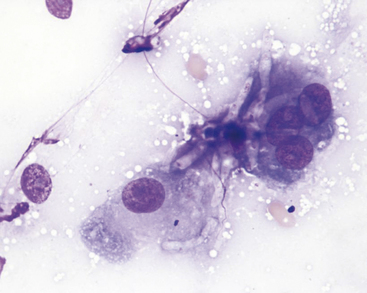
Osteomyelitis is also a relatively common manifestation of coccidioidomycosis and the organisms may be detected in the exudate. The exudate in Coccidioides immitis infections is typically more mixed than that in bacterial infections and often contains a much larger component of activated macrophages and multinucleate giant cells. Other fungal organisms, including Blastomyces dermatitidis and Histoplasma capsulatum, may produce osteomyelitis with a similar exudates.3 Hyphating fungal organisms such as Aspergillus spp. can also be seen and appear as staining or nonstaining fungal hyphae (Figures 13-2 and 13-3).
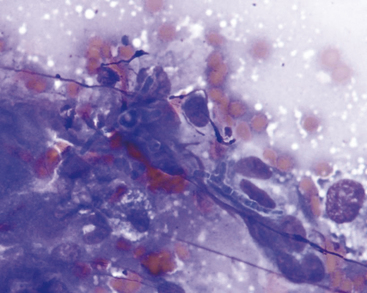
Figure 13-2 Fungal hyphae from lytic bone lesion in a dog. Aspergillus was cultured from this lesion. (Wright’s stain.)
NEOPLASTIC DISEASES
Tumors of Bone
Osteosarcoma
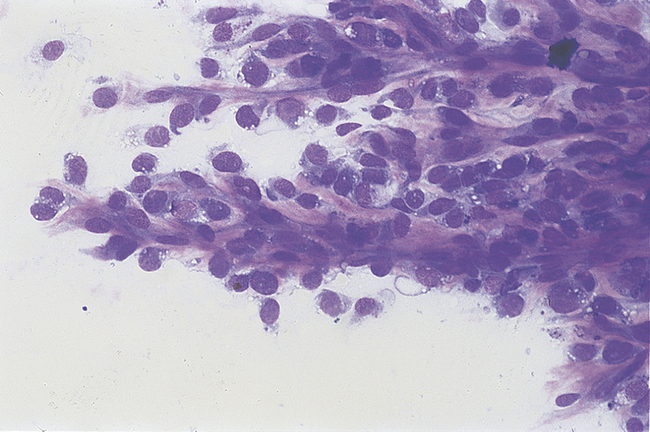
Osteosarcoma is the most common primary bone tumor, and the appendicular skeleton is more commonly affected. In the dog, osteosarcoma occurs more commonly in the front limbs with the distal radius and proximal humerus as the most common sites.4 Aspirates of osteosarcomas are often more highly cellular than aspirates of soft tissue sarcomas. Cells may occur singly or in clusters. One characteristic feature that may be evident on low-power examination of the slide is the presence of islands of osteoid surrounded by tumor cells.5,6 Osteoid (Figure 13-4) appears as a somewhat fibrillar, bright pink material on Wright’s-stained slides. These structures are not found in most aspirates from osteosarcomas; however, when found, their presence provides strong evidence that a tumor is of bone origin. Individual tumor cells vary from round to plump to fusiform, and often vary greatly in size (Figure 13-5). They often have many of the classic cytologic features of malignancy, such as karyomegaly, anisokaryosis, large nucleoli, and multiple nucleoli that differ in size (see Chapter 2). Cytoplasm is typically dark blue and may contain several clear vacuoles (Figure 13-6). A proportion of the cells from most osteosarcomas contain scattered, pink cytoplasmic granules (Figure 13-7). These granules are not specific to osteosarcomas; similar granules may also occur in cells from chondrosarcomas and, less commonly, from fibrosarcomas. Cells from more differentiated osteosarcomas (Figure 13-8) are more uniform and may be difficult to distinguish from normal osteoblasts. Small numbers of inflammatory cells, nonneoplastic osteoblasts, and osteoclasts similar to those described in the previous section on inflammation may also be found in aspirates from osteosarcomas.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


