CHAPTER five The Skull and Vertebral Column
THE SKULL
Anatomy
Lateral View
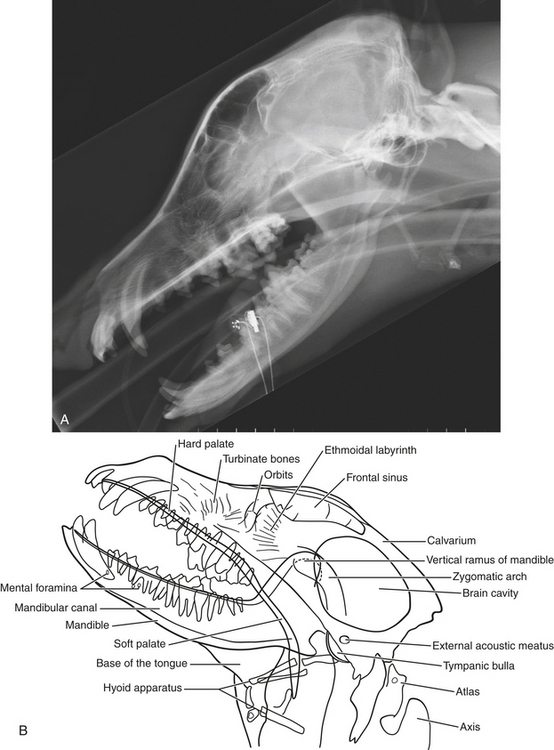
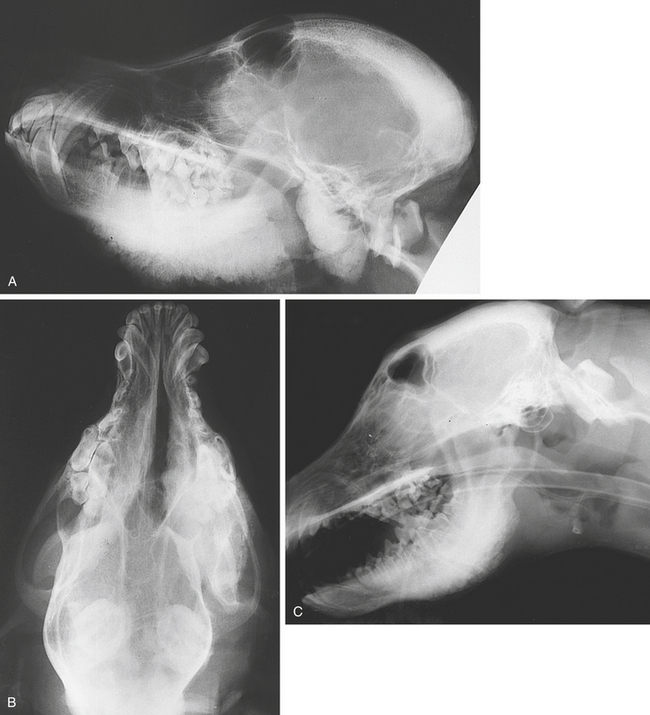
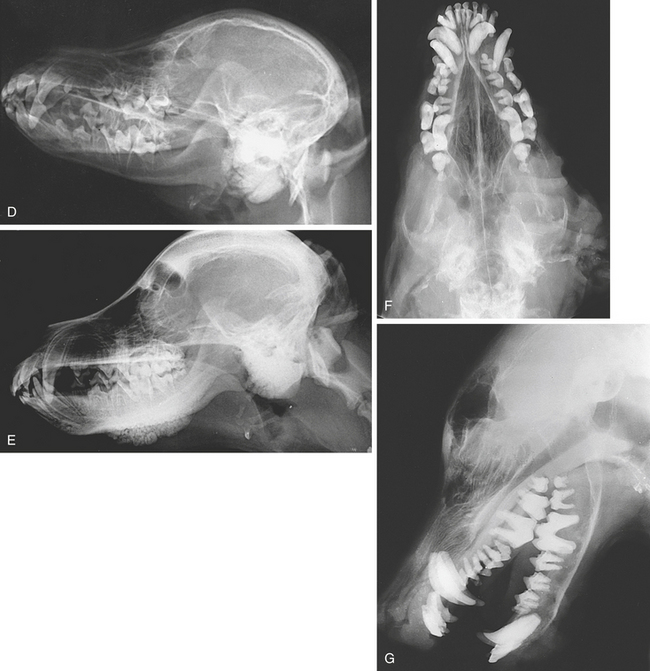
The patient is placed in lateral recumbency. A foam wedge is placed under the animal’s nose and mandible so that the sagittal plane of the skull is parallel to the tabletop. The beam is centered midway between the ear and the eye, dorsal to the zygomatic arch (LeRtL or RtLeL). The jaws should be opened if the temporomandibular joints are the areas of interest (Figure 5-1, A, B, and I).

Ventrodorsal View
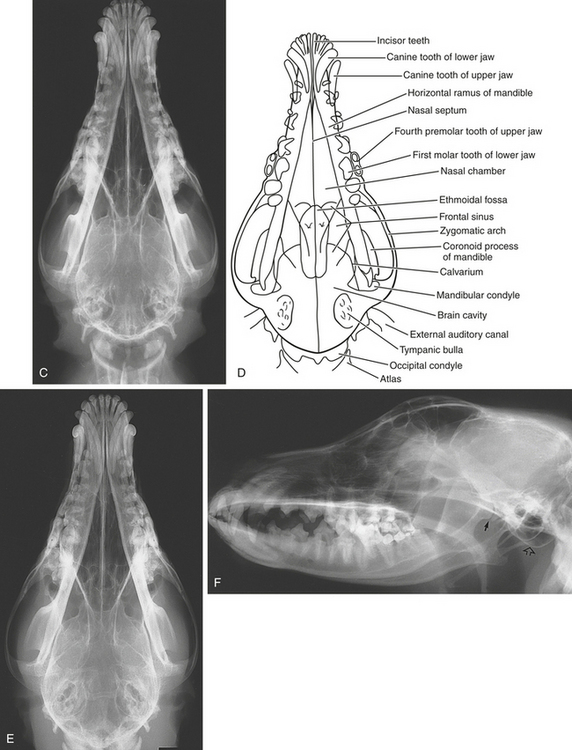
The animal is placed in dorsal recumbency. A radiolucent block is placed under the neck behind the skull. The occipitoatlantal articulation is extended so that the hard palate lies parallel to the film. The x-ray beam is centered between the eyes and the ears on the midline. The sinuses are more clearly seen on this view than on the dorsoventral view, although it is more difficult to achieve symmetry in the ventrodorsal position. This view is best for demonstrating the cranium because the calvarium is closer to the film (Figure 5-1, C and D).
Dorsoventral View
The animal is placed in sternal recumbency with the head resting on the cassette so that the hard palate lies parallel to the tabletop. This position can be maintained by a bandage passed across the neck, behind the skull, and fixed to the table. On occasion it may be easier to position the head if the cassette is raised off the tabletop on a support. The x-ray beam is centered between the eyes and the ears on the midline. It is easier to achieve symmetry in this position than it is in the ventrodorsal position, but the calvarium is farther from the film and is therefore more distorted on this view. However, this is of no practical significance (Figure 5-1, E).
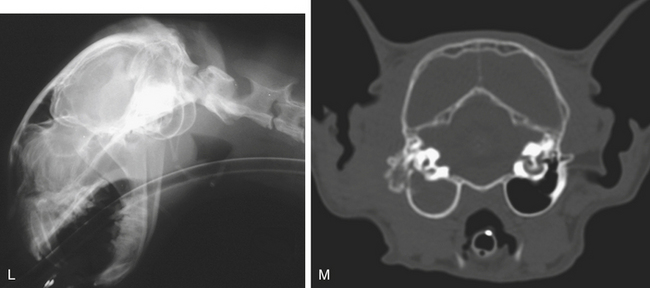
The maxillary nasal turbinates can also be examined in this position by introducing the intraoral film corner first and placing it as far back in the mouth as possible. Alternatively, a high-detail single-screen film combination in a plastic lightproof envelope can be used (Figure 5-1, L). The x-ray beam is centered over the nasal septum. This position can be used with intraoral film to demonstrate the maxillary incisor teeth. The x-ray beam is directed rostrocaudally at an angle of 20 degrees (D20°R-VCdO).
Oblique Views
Oblique views enable some structures to be demonstrated without superimposition of the contralateral side. Oblique views are used to study the temporomandibular joints, the osseous bullae, the frontal sinuses, and the dorsal edge of the orbit. In the open-mouth position, the maxillary and mandibular dental arcades are profiled by using oblique views. The structure profiled varies with the oblique study selected (Figure 5-1, F and K).
Specific oblique views for various anatomic and pathologic abnormalities are discussed in subsequent sections.
Rostrocaudal (Frontal) View
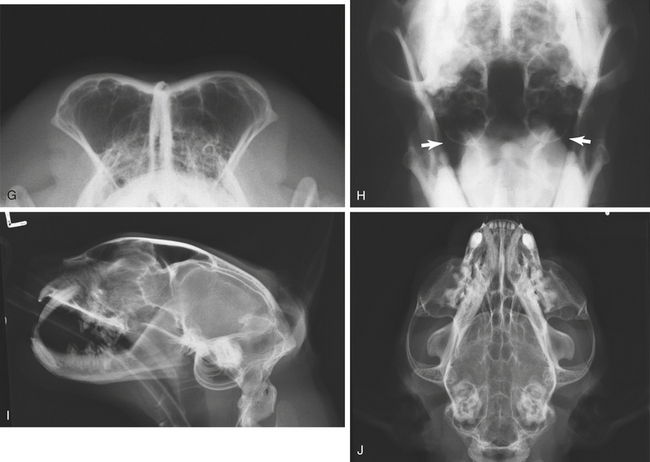
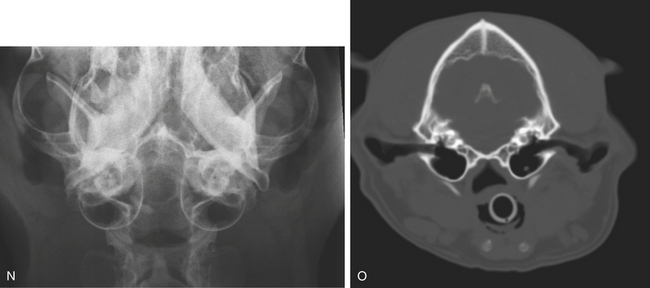
The patient is placed in dorsal recumbency, and the neck is flexed so that the hard palate lies perpendicular to the film. The patient’s head is held in position with a bandage or tape around its nose. The beam is directed at right angles to the tabletop, along the line of the hard palate and centered between the eyes (RCd). The frontal sinuses, the odontoid process or dens, and the foramen magnum can be demonstrated on this view. In cats, a similar technique can be used to demonstrate the tympanic bullae, which lie ventral to the mandibles. The patient is placed in dorsal recumbency, and the head is flexed. Rather than being oriented with the hard palate perpendicular to the tabletop, the head is tilted slightly dorsal so that the hard palate is at an angle of approximately 70 to 80 degrees to the tabletop and the beam centered just ventral to the mandibular symphysis (Figure 5-1, N). This frontal view, with the animal’s mouth opened, can be modified to demonstrate the osseous bullae and temporomandibular joints, in which case the beam is directed rostrocaudally at an angle of 20 to 30 degrees to the hard palate (Ro20°V-CdDO). By varying the angles of the hard palate to the tabletop, the frontal view can also be used to outline the calvarium (Figure 5-1, G and M; also see Figure 5-13, C and F).
Normal Appearance
The appearance of the normal skull is best demonstrated by illustrations (see Figure 5-1).
Abnormalities
Because the bone structures are bilaterally symmetric, a skull examination frequently makes it possible to compare a unilateral abnormality with the corresponding normal structure on the opposite side.
Fractures
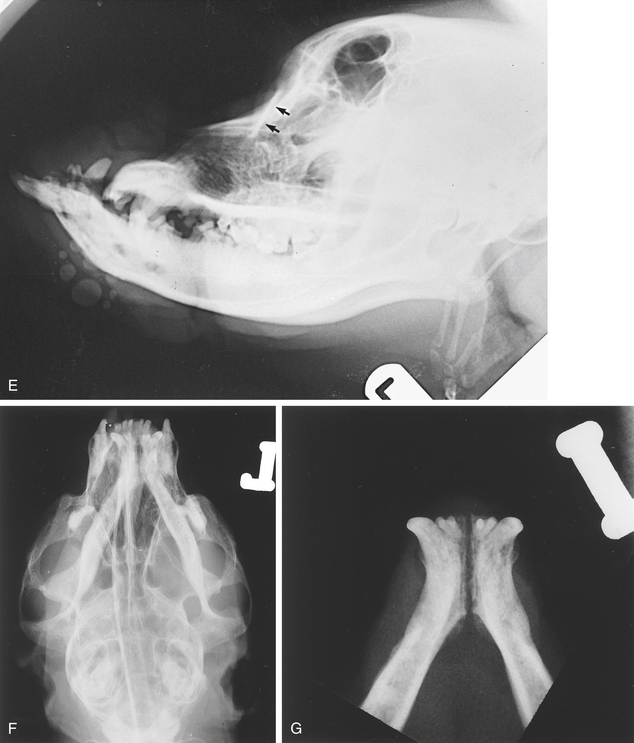
Skull fractures in dogs are not very common except for fractures of the mandibles. The superimposition of bones makes fractures difficult to demonstrate. Lateral oblique views are useful in outlining the mandibular rami. The mandibular symphysis is frequently the site of a separation injury in cats that have fallen from a height (Figure 5-2, G). Fractures involving the calvarium, frontal bones, or nasal bones are often depression fractures, and lesion-oriented oblique (tangential) views of the area may be necessary to demonstrate them. Overriding of fracture fragments may cause a linear opacity, whereas a fracture with displaced ends causes a linear radiolucent defect. Soft tissue swelling is often present. Fractures may be the cause of focal cranial nerve dysfunction. Fractures involving the nasal or frontal bones may be accompanied by hemorrhage into the frontal sinus or nasal cavity. The hemorrhage causes a soft tissue opacity within the air-filled cavity (Figure 5-2).

Temporomandibular Dislocation
Traumatic luxation (Figure 5-3, D) of the temporomandibular joint is not very common in dogs. It may be associated with mandibular fracture, particularly in cats. Clinically, affected animals hold the mouth open, and manipulation of the mandible is painful. The dislocation is usually unilateral. The displaced mandibular condyle can be seen radiographically on the appropriate view. It is seen to be displaced rostrally and dorsally from the retroglenoid (retroarticular) process. If the dislocation is unilateral, comparison with the opposite side is helpful. The mandibles are displaced toward the normal side. There may be an associated fracture. If the retroglenoid process is fractured, the condyle may displace caudally.
Foreign Bodies
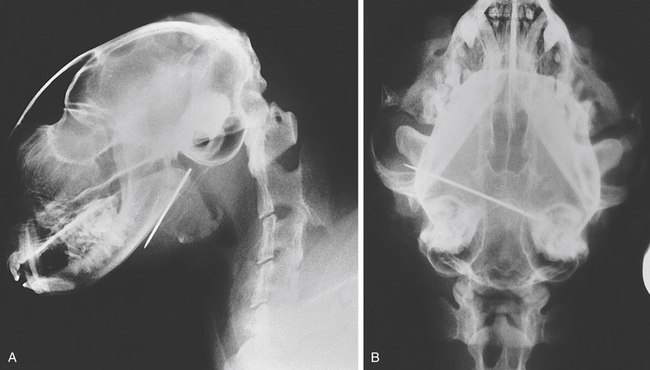
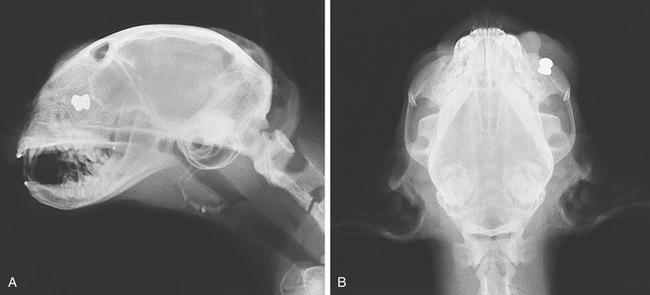
Radiopaque foreign bodies are readily seen within the skull. They are usually located in the mouth, pharynx, or nasal chambers. Radiolucent bodies may require contrast medium to outline them (Figures 5-4 and 5-5; see Figure 5-11).
Infection
Radiologic Signs
Neoplasia
Primary neoplasia of skull bones is not common. The dog is more often affected than the cat. Osteosarcoma may affect any of the bones of the skull. Its appearance is that of a destructive lesion, usually accompanied by a profuse and aggressive periosteal reaction. If the tumor is superficial, there will be an associated soft tissue swelling. Proliferative changes and sclerosis are more prominent than are erosive changes when the cranial vault is involved. Other neoplasms, such as fibrosarcoma, chondrosarcoma, and osteochondroma, are occasionally seen.
An effort should be made to rotate the skull for a lesion-orientated view so that the mass lesion is as near to the film as possible and there are few superimposed structures (Figure 5-6).


Caudal Occipital Malformation Syndrome: Congenital Malformation of the Foramen Magnum (Occipital Dysplasia, Chiari Malformation)
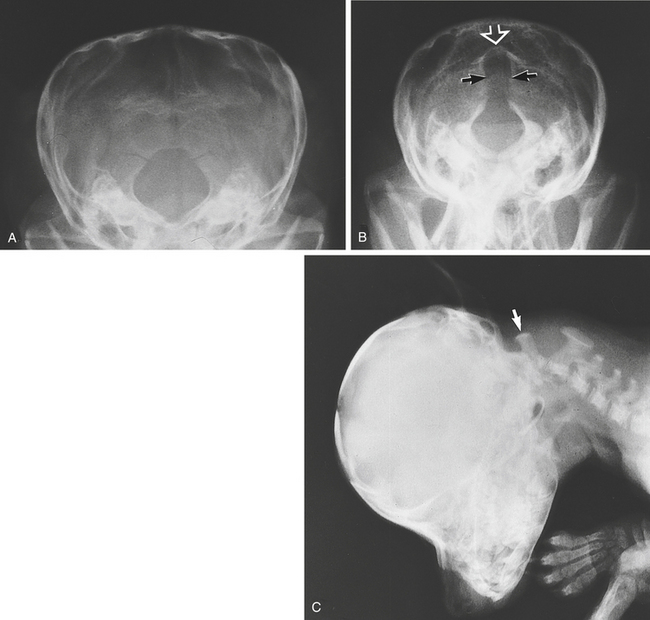
Caudal occipital malformation syndrome is a congenital anomaly of the occipital bone. The foramen magnum is formed in the occipital bone. Congenital malformation of the foramen magnum occurs in small and toy dog breeds. The foramen magnum is enlarged dorsally and is abnormal in shape. It has been described as having a “keyhole” appearance. In the normal animal the shape of the foramen magnum varies, making it difficult to evaluate the exact shape of the foramen without the use of CT or MRI. The thin plate of bone at the dorsal aspect of the foramen is virtually radiolucent. Radiographically, this may give the appearance of an enlarged foramen. The condition is believed to occur as a result of mismatch of the cerebellar and caudal fossa volumes, which leads to increased intracranial pressure. This causes part of the cerebellum to be herniated through the foramen magnum. The cerebellar herniation obstructs flow of cerebrospinal fluid (CSF) to the subarachnoid space of the spinal cord, resulting in reduced pressure in this space. High-velocity pulsatile flow of CSF into the central canal of the spinal cord leads to hydromyelia or syringomyelia. Hydromyelia is dilation of the central canal of the spinal cord. Syrinxes are fluid-filled cavities that may be continuous or segmental, tubular or saccular, and are seen in the cervical and sometimes in the cranial part of the thoracic spinal cord. There may also be dilation of the lateral and third ventricles.
Clinical signs are variable. Some dogs are apparently normal; others may show pain, obsessive scratching, ataxia, and quadriparesis. Ataxia has been reported in approximately 25% of cases with enlarged foramen magnum. The brainstem and cerebellum can herniate through the enlarged foramen, giving rise to neurologic signs. There may be an associated hydrocephalus with open suture lines. Cisternal puncture for CSF collection or myelography is contraindicated in dogs in which cerebellar herniation may occur. MRI is the imaging method of choice. Sagittal plane T1- and T2-weighted images are most helpful. The caudal border of the cerebellum appears flattened, and part of the cerebellum is herniated through the foramen. Syringomyelia and hydromyelia appear as tubular hypointense structures within the spinal cord on T1-weighted images and hyperintense structures on T2-weighted images (see Figure 5-32 and p. 510).
A number of other abnormalities are encountered in this area. The first cervical vertebra may be shortened, and there may be hypoplasia and nonfusion of the odontoid process (dens). The significance of anatomic changes seen in this region is often uncertain. A lateral view of the cervical spine is required to demonstrate these changes (Figure 5-7).
There may be an accompanying hydrocephalus and syringomyelia or hydromyelia.
Craniomandibular Osteopathy (Craniomandibular Osteoarthropathy, Mandibular Periostitis, Craniomandibular Osteodystrophy, “Lion Jaw”)
Craniomandibular osteopathy produces proliferative changes, particularly on the mandible and in the areas of the osseous bullae. The calvarium may be thickened. New bone formation at the distal metaphyses and along the diaphyses of the radius and ulna has been reported, although this is rare.
Radiologic Signs
The temporomandibular joints are rarely directly involved in the new bone growth, but their movement may be inhibited because of the bony masses around them (Figure 5-8, A to E).
Renal Secondary Hyperparathyroidism (“Rubber Jaw,” Renal Osteodystrophy, Renal Rickets, Renal Osteitis Fibrosa)
A secondary hyperparathyroidism in older animals may result from renal insufficiency caused by chronic renal disease. It is occasionally seen in young animals with congenital nephropathies. In short, if the glomerular filtration rate is reduced, there is retention of phosphorus and resulting progressive hyperphosphatemia. The hyperphosphatemia causes a lowering of the blood calcium level, which provokes hyperparathyroidism. The resulting increase in parathyroid hormone levels causes a resorption of bone and a release of calcium. The skull is primarily involved with demineralization of the mandible and the maxilla. Demineralization elsewhere is slower. Clinically, the mandible becomes softened (rubbery), teeth become loose, and breathing may be impaired because of collapse of bones around the nasal cavity. The face may appear swollen as a result of proliferation of fibrous tissue. Salivation is common.
Radiologic Signs
THE NASAL CHAMBERS
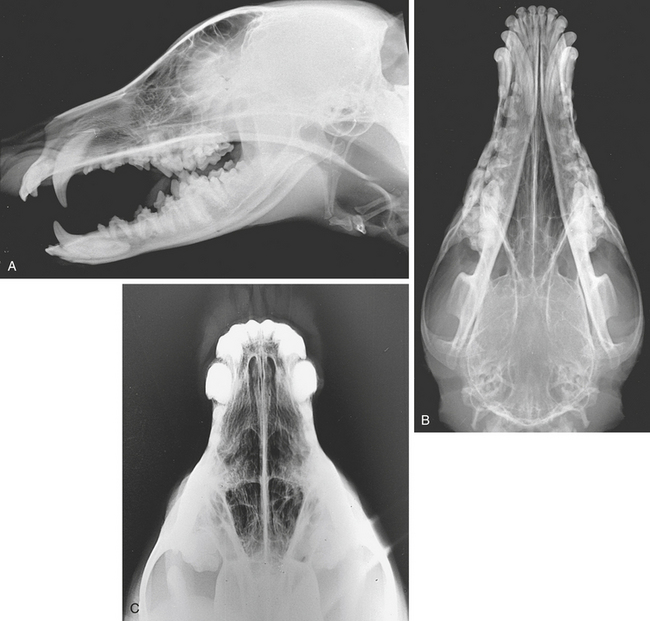
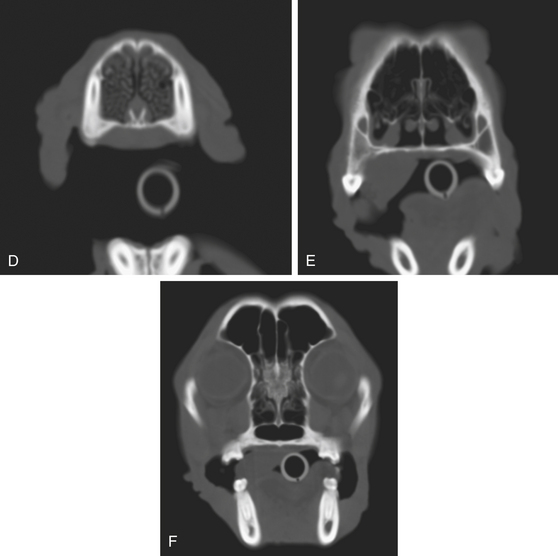
Normal Appearance
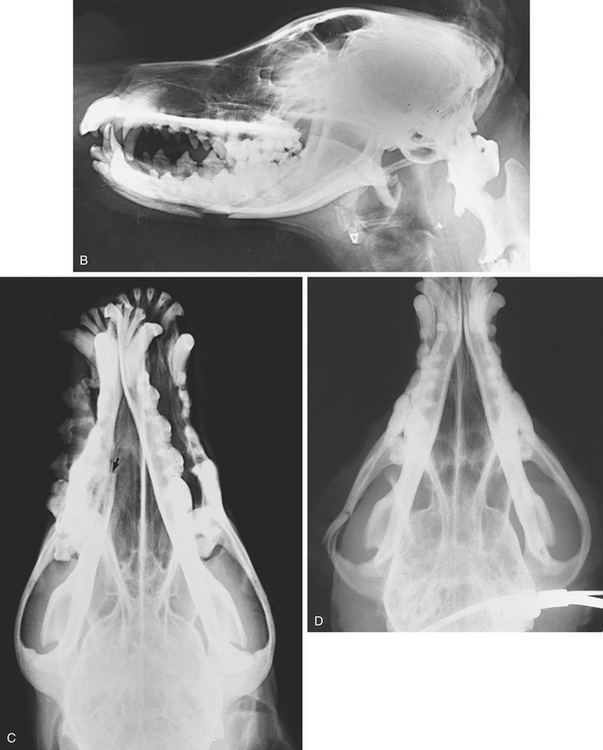
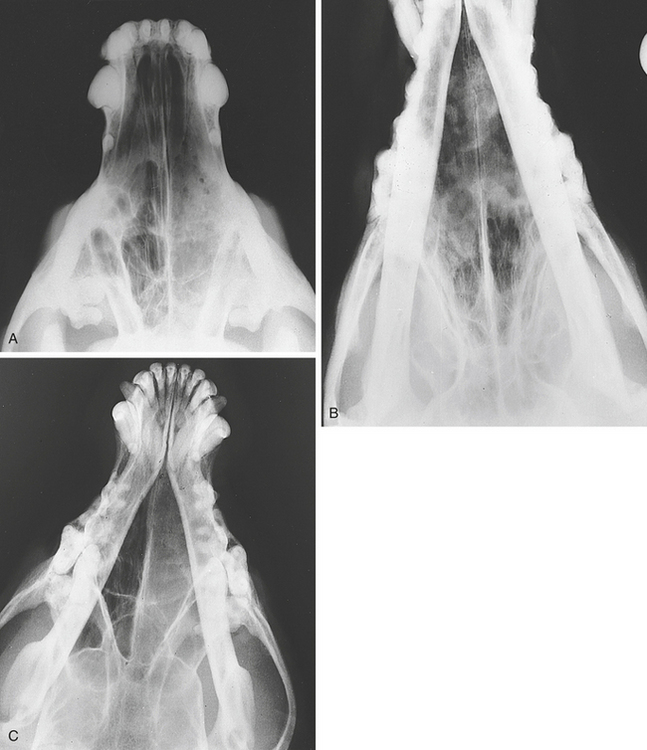
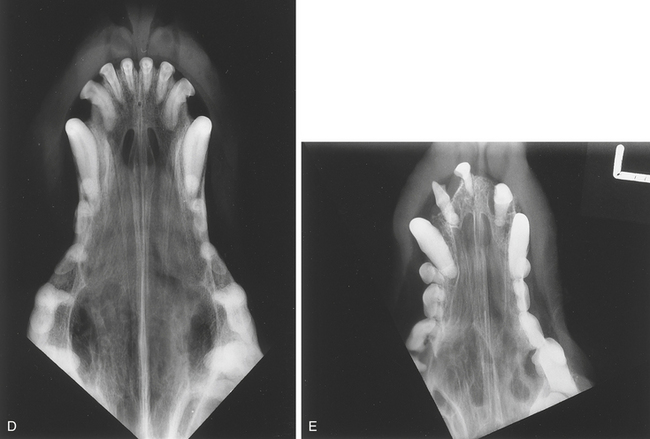
The nasal chambers normally project a fine, bony, trabecular, or turbinate pattern surrounded by lucent nasal cavities. The nasal septum divides the nasal cavity into two symmetric halves (Figure 5-9).
Abnormalities
Infection
Aspergillosis
Areas of decreased opacity within the nasal chambers have been reported in association with aspergillosis. This is a destructive rhinitis seen mainly in young doliocephalic types of dog. The nasal septum may be destroyed. The lesions often start rostrally in the nasal cavity. The infection causes necrosis and sloughing of the conchae and the nasal mucous membrane. In chronic cases, punctate lytic lesions are sometimes seen in the maxillae and nasal bones, but they are not pathognomonic for aspergillosis. If there is extension into a frontal sinus, it acquires a granular, mottled opacity. Destructive rhinitis may disrupt the vomer bone. It can be difficult to differentiate destructive rhinitis from neoplasia when there is mucosal thickening, accumulated exudate, and hemorrhage and fungal granulomas. However, some cases have complete turbinate destruction and marked hyperlucency of the nasal chambers, which are characteristic of the condition. Less commonly, other organisms, notably Penicillium spp., may cause destructive rhinitis.
Cryptococcosis
This fungal infection occurs most commonly in cats, although other species may be affected. The nasal cavities, the paranasal sinuses, and occasionally the lungs are involved. The pigeon is a common vector. Clinical signs include sniffling and sneezing, with a unilateral or bilateral nasal discharge. Oral ulceration is occasionally present. Skin nodules with or without ulceration are common. The central nervous system may be involved through spread from the nose through the cribriform plate of the ethmoid bone. Radiographically, there is an increased opacity within the nasal chambers with occasional bone erosion and involvement of the frontal sinuses. Cryptococcosis usually results in a hyperplastic reaction rather than a destructive one.
Rhinitis may be caused by dental disorders. Rhinitis and sinusitis in the cat may occur from viral infection. Otitis media has been reported as a sequela (Figure 5-10).
Foreign Body
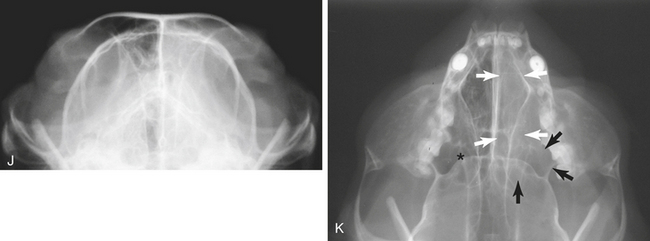
Radiopaque foreign bodies are readily recognized on radiographs. The skull should be examined as far caudally as the pharynx. Clinically, there may be sneezing and a nasal discharge. Radiolucent foreign bodies are not seen. However, there may be increased opacity within the affected chamber as a result of inflammatory exudate. The introduction of contrast medium into the nasal chamber (contrast rhinography) is seldom informative, except perhaps in the case of a large radiolucent foreign body (Figure 5-11).
Neoplasia
Radiologic Signs
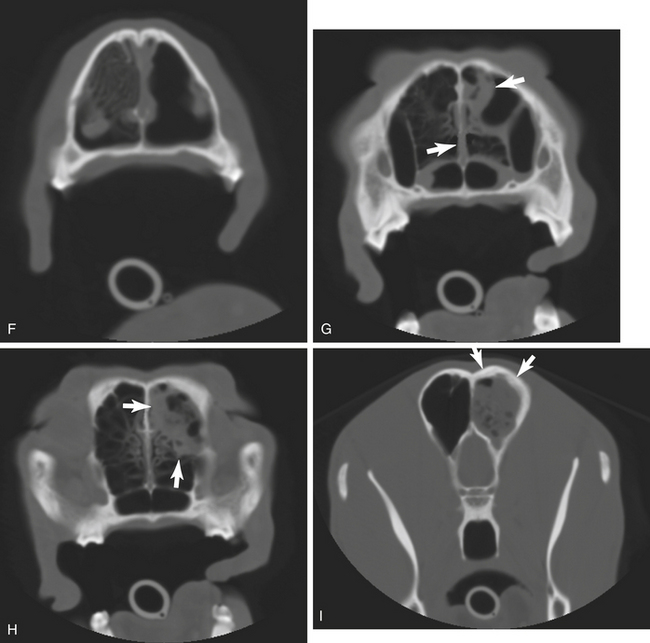
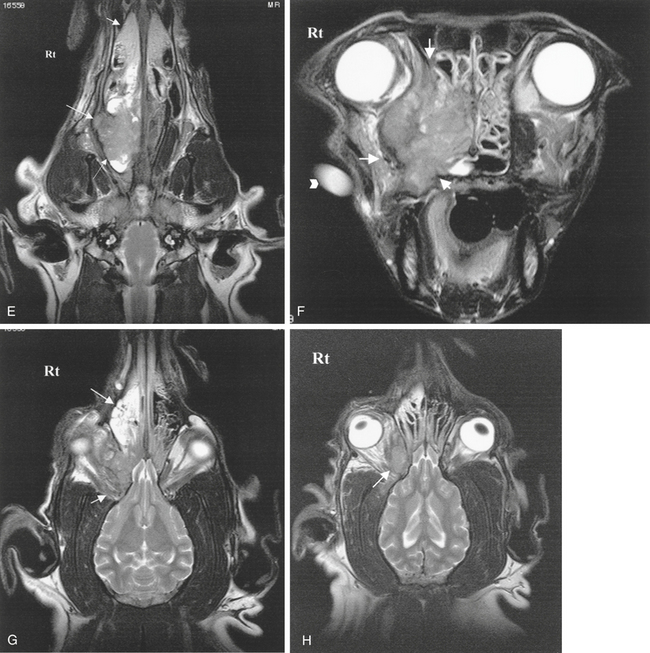
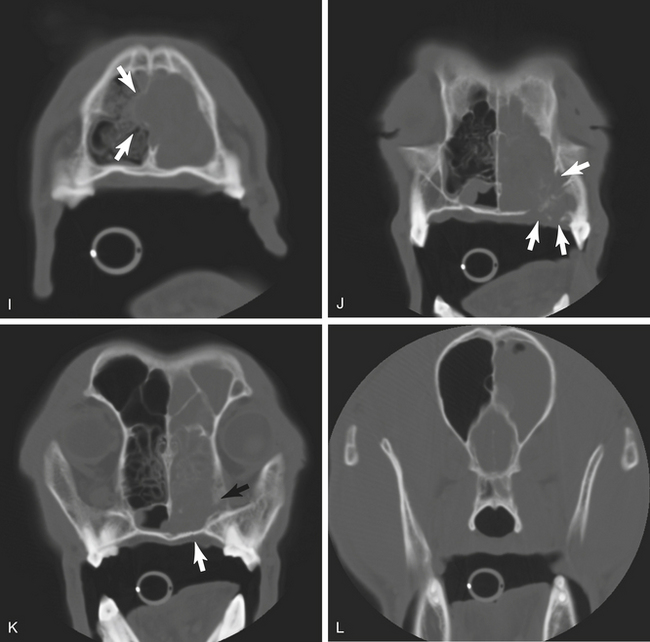
Because the radiologic signs of infection and neoplasia are similar in many respects, it is usually impossible to be sure on radiographic evidence alone whether the cause is infection or a neoplasm. This is particularly true in cats. Some infections can be very destructive, such as aspergillosis. If there is an associated soft tissue mass, there is a strong presumption that the lesion is neoplastic. CT and MRI are useful to evaluate fully the precise area and extent of the lesion (Figure 5-12).
THE PARANASAL SINUSES
Normal Appearance
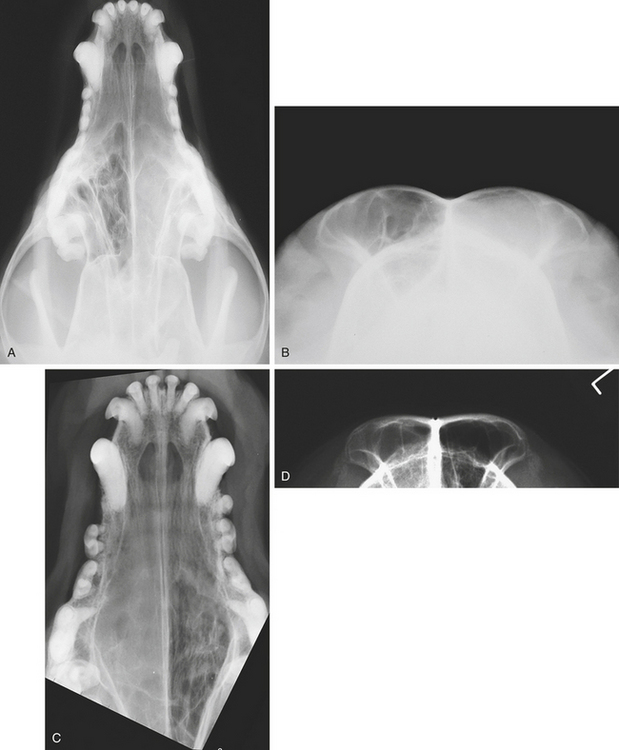
On the lateral view, the frontal sinuses are clearly seen, superimposed on one another above the orbit. They have an air opacity, and fine bony septa are visible within them. Both sinuses are seen individually on the rostrocaudal or caudorostral view. On ventrodorsal and dorsoventral views of the skull, a portion of each sinus is seen just rostral to the cranium. The maxillary and ethmoid sinuses are not usually identifiable on radiographs (Figure 5-13, A to C).
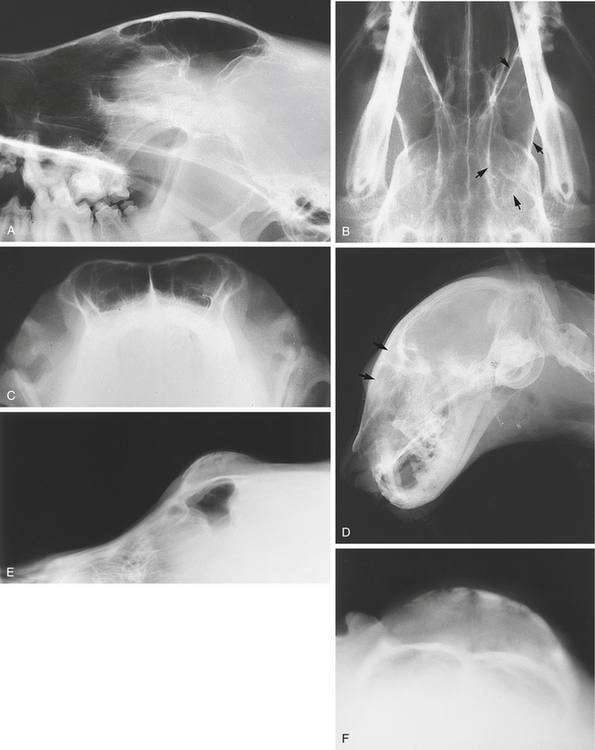
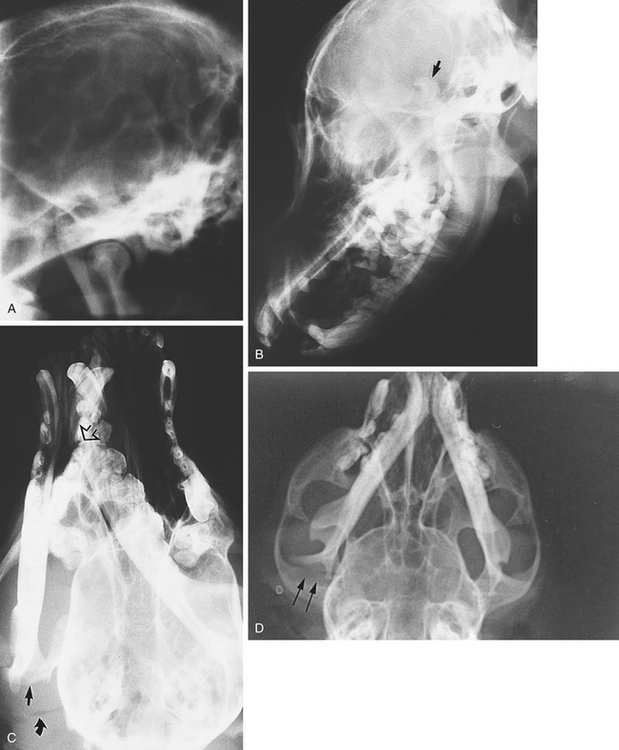
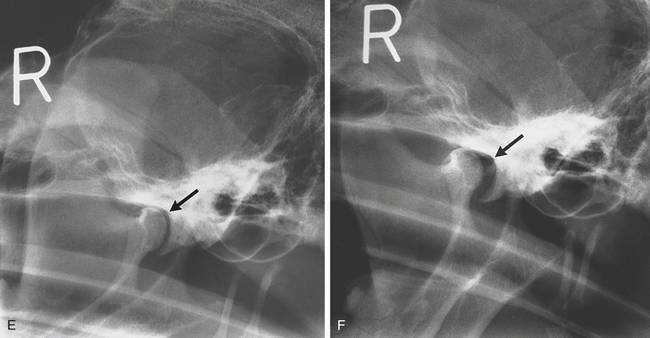
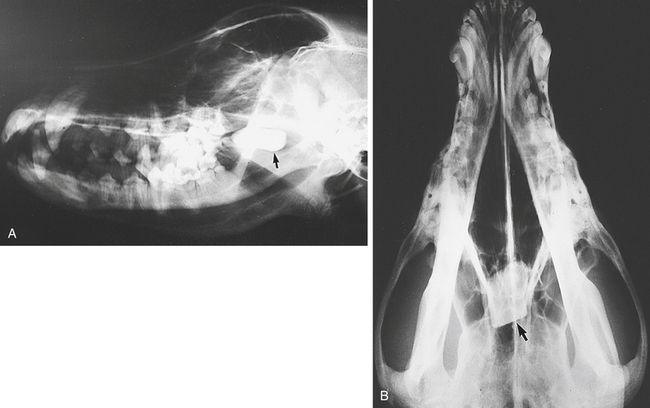
Figure 5-13 Normal frontal sinuses (see Figure 5-1). A, Lateral view. B, Ventrodorsal view. Arrows mark the outline of the left frontal sinus. C, Rostrocaudal view. D, The normal air opacities of the frontal sinuses (arrows) of this cat have been lost because of infection. E and F, A 7-month-old Collie with a hard swelling over the midfrontal sinus area. Lateral (E) and rostrocaudal (F) views show an expansile soft tissue mass extending dorsally with a mineralized rim. This was a cyst in the frontal sinus. This is a benign condition.
Abnormalities
Infection
With infection in a frontal sinus, the normal air opacity within it is replaced by a fluid or soft tissue opacity (Figure 5-13, D). Unless the condition is of long standing, there is usually no associated bone abnormality. Thickened mucous membranes may be visible within the sinus. Infection may reach the sinus from the nasal chambers. Fluid may occasionally be seen on a horizontal beam caudorostral view. A horizontal line is evident at the air/fluid interface. Infection in a maxillary sinus, such as that associated with malar abscess, is not readily demonstrable radiographically unless there are associated bone changes. Expansion of the frontal sinus may be caused by a cyst in the sinus (Figure 5-13, E and F). Obstructive sinusitis is a common sequela to primary nasal neoplasia in dogs.
Neoplasia
Neoplasia affecting the frontal sinus causes loss of the normal air opacity within the sinus. The tumor mass replaces the air. Invasion of the surrounding bone, with destruction and periosteal reaction, becomes evident as the condition progresses. The frontal bone may be a site of osteosarcoma. Squamous cell carcinoma is the most common primary soft tissue tumor. Adenocarcinoma also occurs. These tumors are highly destructive, and considerable erosion of bone may have occurred before they are detected. Invasion of the sinuses by tumors arising in the nasal cavity is more common than primary sinus tumors (Figure 5-14, A and B).

THE AUDITORY SYSTEM
Radiography
Dorsoventral, oblique, open-mouth views and the caudorostral view in cats are used to study the auditory system. In cats a modification of the rostrocaudal view for profiling the tympanic bullae has been reported. The mouth is closed and the head tilted caudally 10 degrees from the vertical; the x-ray beam is aligned perpendicular to the tabletop and centered just ventral to the nares (R10°V-Cd DO) (see Figure 5-1).
Positive Contrast Ear Canalography
This technique may occasionally be useful when it is difficult or impossible to visualize the tympanic membrane directly. In many cases this procedure is unrewarding and of limited value. The dog is placed in lateral recumbency with the affected ear uppermost. The ear canal should be gently cleansed. Iopamidol or iohexol is diluted with an equal volume of normal saline. The ear canal is filled with the mixture. The contrast material is massaged along the length of the vertical and horizontal canals. The ear is plugged with cotton wool or a cotton ball, and radiographs of the area are made. If the tympanic membrane is ruptured, contrast material will leak into the tympanic bulla. If the horizontal canal is occluded with debris, the procedure may prove nondiagnostic. The ear should be flushed out after the procedure to remove the contrast agent. Ultrasonography of the tympanic bullae has been reported as useful in assessing the presence of fluid or air within the bullae.
Abnormalities
Otitis Externa
Otitis Media
Avulsion of the Auditory Canal
Nasopharyngeal Polyp
In cats a polyp sometimes extends on a stalk from the eustachian tube into the pharynx and nasal cavity, which it may obstruct. The presenting signs are nasal discharge, sneezing, and stridor.
Neoplasia
Neoplasia arising in the external ear canal, particularly squamous cell carcinoma or adenocarcinoma, may cause bone destruction in the area of the tympanic bulla and petrosal part of the temporal bone. There is usually an associated soft tissue swelling. Neoplasia may also affect the middle ear and the tympanic bulla (Figure 5-14, J).
Craniomandibular osteopathy may cause proliferative bony changes in this region that should not be mistaken for neoplasia (see Figure 5-8, A to E).
THE EYE
As an incidental finding, opacification of the lens (cataract) can be seen lying rostromedial to the caudal root of the zygoma. Cataracts are often bilateral and should not be mistaken for foreign bodies (see Figure 5-6, G).
Ultrasonography
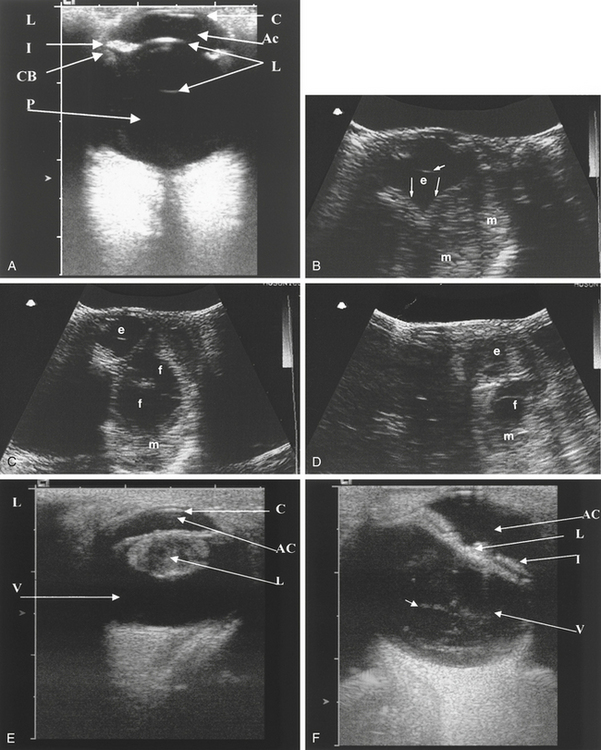
Horizontal and sagittal (longitudinal) plane sections should be obtained and the transducer swept gently in dorsoventral and mediolateral directions. The small groove or mark on sector, convex, and microconvex transducers indicating the plane of section helps orientation of the ultrasound beam. This groove should be kept at the lateral aspect of the eye when scanning in a transverse plane and at the dorsal aspect of the eye when scanning in a sagittal plane (Figure 5-15, A).
Anatomy
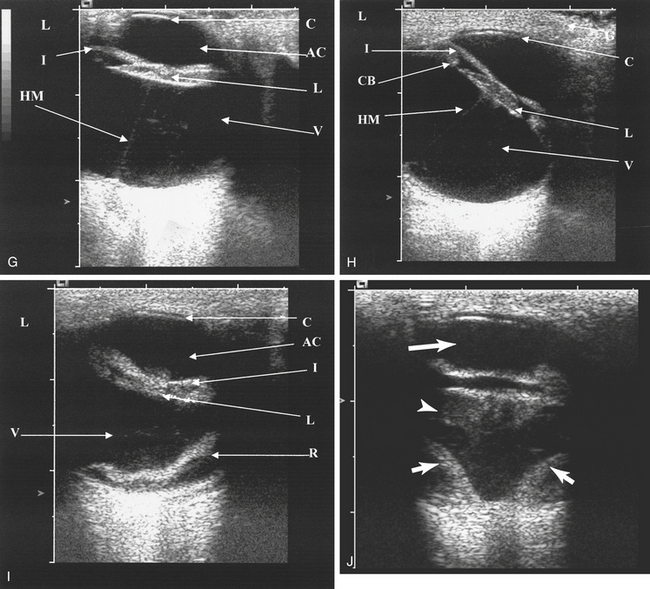
The eye is spherical, smooth, and well defined. The cornea is examined by using a standoff and is identified as a smooth, hypoechoic, well-marginated structure lying in the near field. With high-frequency transducers, three layers are usually visible within the cornea. The anechoic anterior chamber lies just behind it. The curved lens is usually anechoic but casts hyperechoic horizontal linear echoes at its anterior (rostral) and posterior surfaces. The ciliary body lies to either side of the lens and can be identified as hyperechoic streaks running laterally and medially. The anterior and posterior vitreous chambers are anechoic, and the curved hyperechoic posterior wall of the globe is seen caudally. The sclera, retina, and choroids cannot be individually recognized. The optic nerve is identified as a small hypoechoic depression in the posterior wall. Retrobulbar tissues are poorly defined. They are identified as a cone-shaped structure running from the back of the globe caudally. They consist of the moderately echogenic fat tissues with the hypoechoic medial rectus muscle lying medially (Figure 5-15, A).
Abnormalities
Cataracts result in thickening of the lens capsule so that the entire circumference becomes visible. There is also increased echogenicity of the lens parenchyma. Intraocular masses disrupt the normal architecture. They have a variable echotexture and displace the vitreous ciliary body and lens. Retrobulbar masses may cause displacement of the posterior wall. They have mixed echogenicity. Differentiation between neoplasia and infection is not usually possible without ultrasound-guided fine-needle aspiration or biopsy. Variable amounts of anechoic or flocculated fluid may be present with either neoplasia or infection (Figure 5-15, B to D). Intraocular hemorrhage causes increased echogenicity in the affected chamber. With time, echoes become organized and form hypoechoic masses.
Deformities or abnormal position of the lens are readily demonstrated (Figure 5-15, E to H). High-frequency transducers of 13 to 15 MHz permit the identification of subtle abnormalities such as persistent hyaloid membrane. This membrane extends from the caudal aspect of the lens to the retina (Figure 5-15, H).
Retinal detachment is seen as a linear arc extending from the posterior wall of the eye rostrally into the vitreous humor. Anechoic fluid lies behind the retinal membrane. If it is completely detached, it forms a curved V centered at the optic disk, where it remains attached (Figure 5-15, I and J). Intraocular or retrobulbar foreign bodies are seen as echogenic structures with variable degrees of acoustic shadowing.
Floating echogenic foci (floaters) are often seen in the vitreous humor. They are of no clinical significance. They should not be confused with resolving hemorrhage or inflammatory exudates (Figure 5-15, F).
THE TEETH
Radiography is of value in the assessment of periodontal and periapical disease and in the demonstration of fractures, neoplasms, foreign bodies, malocclusion, and other abnormalities (see Figure 5-18).







