CHAPTER six Soft Tissues
CALCIFICATION (MINERALIZATION)
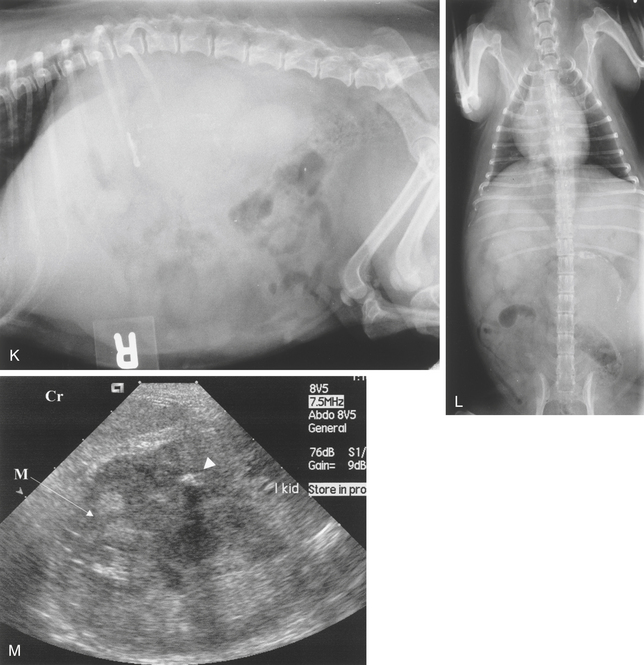
Calcification is a process by which calcium salts are deposited in tissue. Dystrophic calcification is the deposition of calcium salts in abnormal tissue or tissue that is dead, degenerating, or damaged. Metastatic calcification is the deposition of calcium salts in tissue that is not the site of a disease process. It results from abnormalities in blood and tissue calcium and phosphate levels. It is associated with such metabolic disturbances as hyperparathyroidism (hypercalcemia) or hypovitaminosis D. Calcific deposits may be found in such soft tissues as the lungs, gastric mucosa, and kidneys (see Chapter 2, pp. 46, 58, and 136), as well as those around joints (see Chapter 4, pp. 420-422, 428, and Figure 4-45, A to C) and in the walls of blood vessels (Figure 6-1).
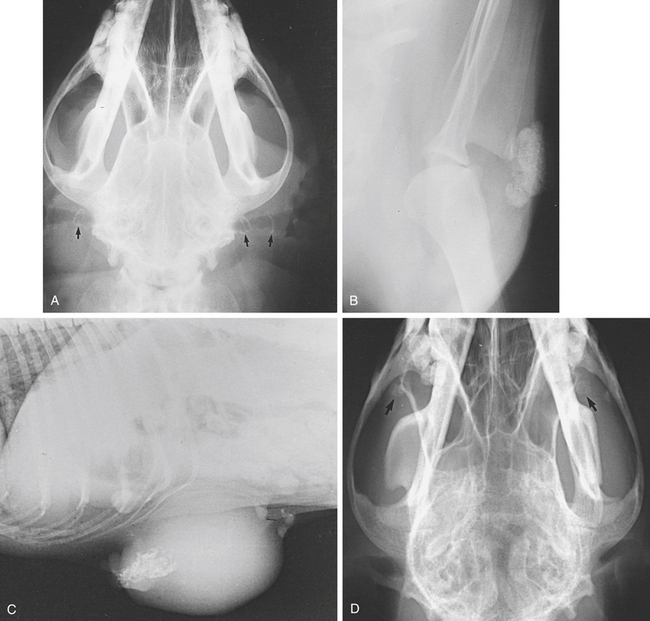
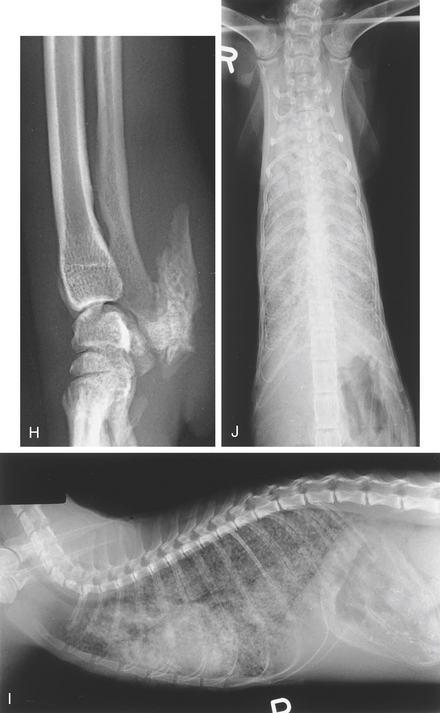
Calcification of the external ear canals may occur in old dogs (Figure 6-1, A). Hematomas or bursae may calcify, as may tumor tissue (Figure 6-1, B). Calcification of the medial meniscus of the stifle has been reported in dogs and cats (see Figure 4-5, B and C).
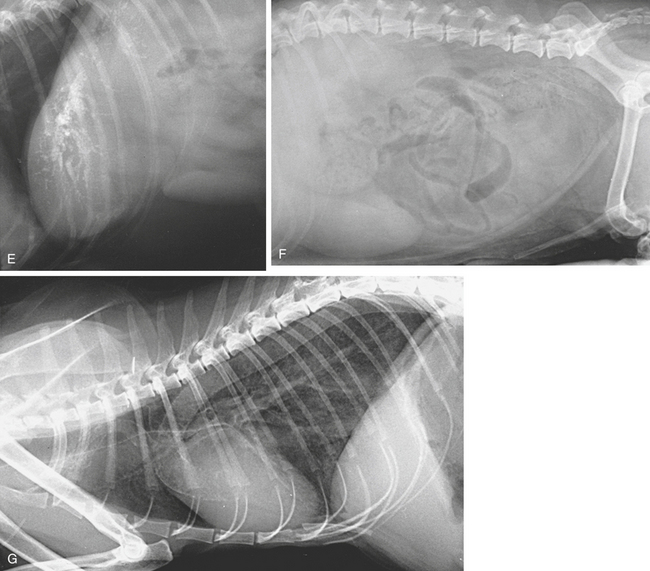
Calcium may be laid down in the skin and subcutis in Cushing’s syndrome (see Chapter 2, p. 123) and secondary to hyperparathyroidism (calcinosis cutis). The tracheal rings and bronchial walls may be affected and there may be diffuse pulmonary parenchymal mineralization (see Figures 3-12, E, and 6-1, F and G).
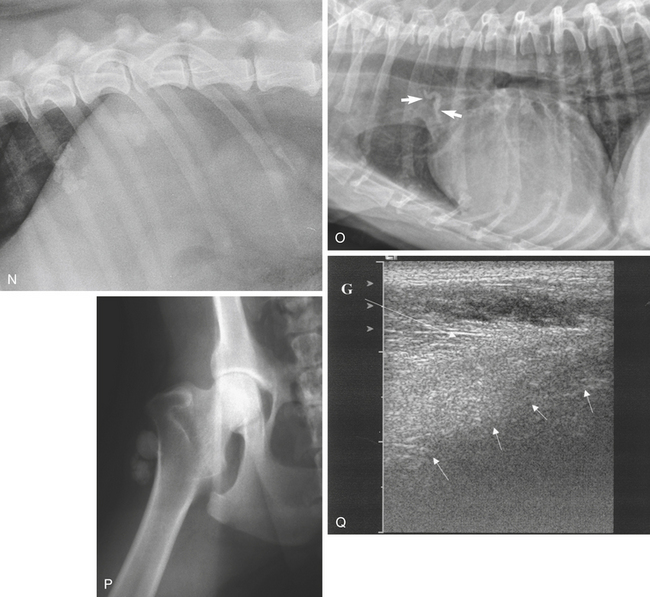
Mineralization of the coronary arteries may be seen as faintly radiopaque lines extending caudoventrally from the aortic root. Mineralization of the aortic bulb is occasionally seen at the level of the fourth intercostal space in the craniodorsal region of the cardiac silhouette (Figure 6-1, O).
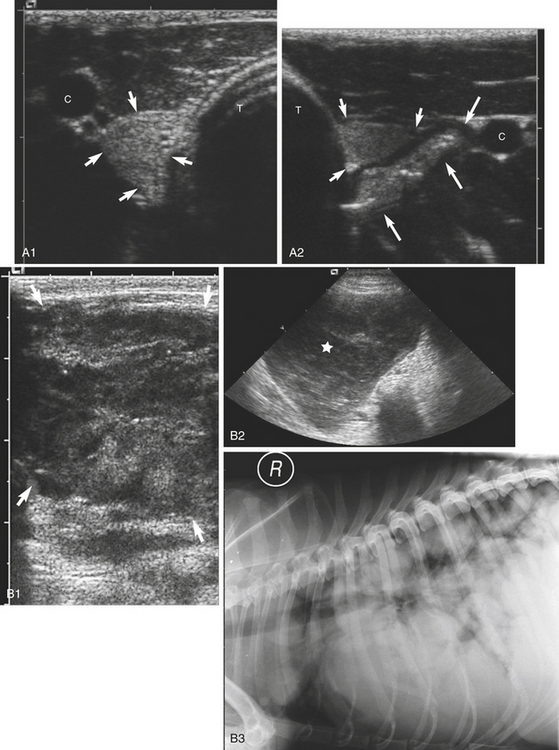
Ultrasonography of calcified tissue can be unrewarding if a structure is only partially calcified. Deposits will be seen as hyperechoic foci scattered in the tissues (Figure 6-1, M). In myositis ossificans, bony plaques are deposited in muscle, or the muscle itself may become ossified. Trabeculated bone opacities may be seen. It may occur as a result of chronic trauma. Calcification cannot be distinguished from ossification unless a trabecular pattern can be identified (Figure 6-1, Q).
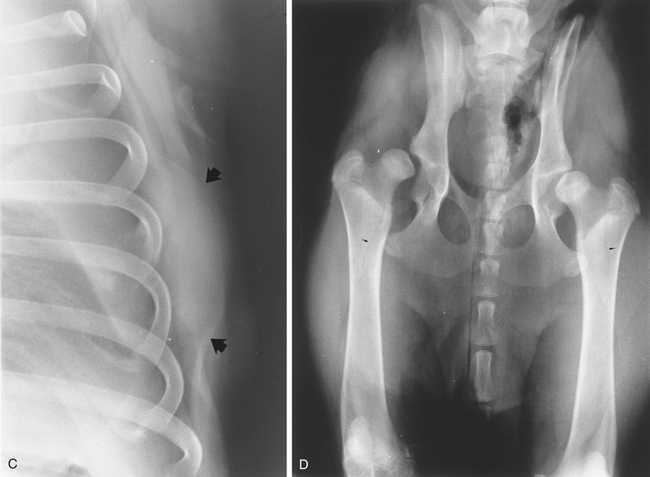
In calcinosis circumscripta (calcium gout, kalk gicht [chalk gout], tumoral calcinosis), deposits of amorphous calcified material are laid down in the subcutaneous tissue and skin. Lesions are usually found on the limbs, under the pads, or over bony prominences. Similar lesions have been described in the mouth. The etiology remains obscure. Chronic renal disease, hyperparathyroidism, and hypovitaminosis D have been suggested as possible causes. Approximately half the cases seen occur in young German Shepherds that are otherwise apparently normal (Figure 6-2).

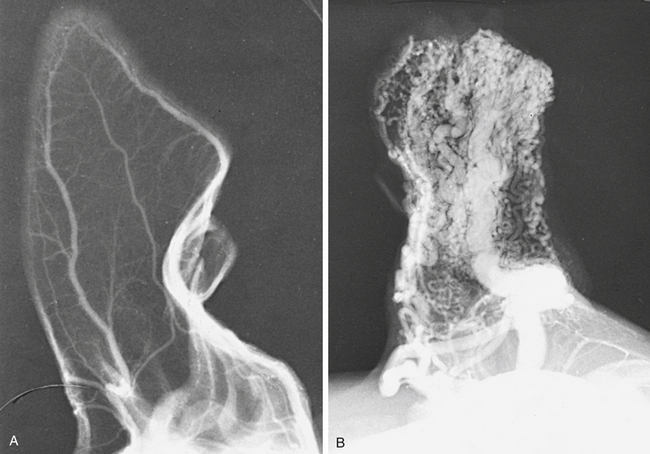
ARTERIOVENOUS FISTULA
Radiologically, arteriovenous fistulas on the limbs may cause alterations in the trabecular pattern of bones in the neighborhood. The trabecular pattern becomes coarse. The vascular bed can be demonstrated by arteriography (Figure 6-3; also see Figure 4-25 and Chapter 4, p. 398).
FASCIAL PLANES
The fascial planes between muscles are frequently visible on radiographs because of the fat that is present in the connective tissue between the muscles. The use of a bright light assists in seeing them (see Chapter 4, p. 361, Figure 4-11, A). If fascial planes are of particular interest, a soft tissue technique is used to demonstrate them. Air may be injected into the subcutaneous fascia, where it will spread to the intermuscular fascial planes and be visible radiographically.
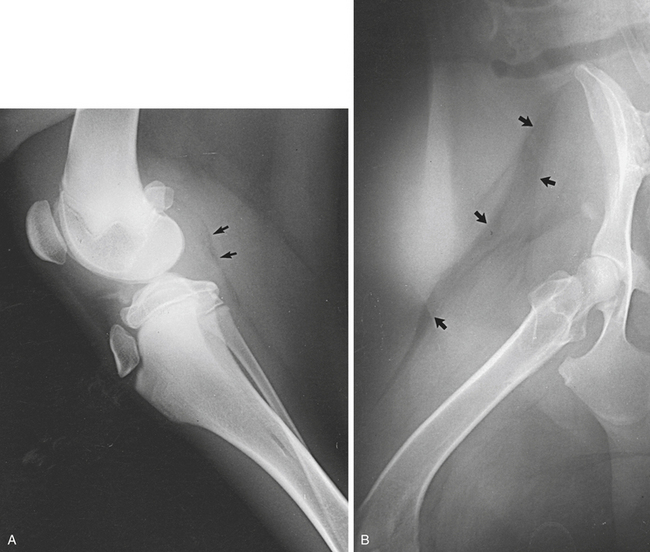
Displacement of fascial planes is of diagnostic significance. For example, displacement of the fascial plane usually visible caudal to the stifle joint indicates intraarticular swelling of the stifle joint. The infrapatellar fat pad may lose its radiolucency if intracapsular hemorrhage or edema is present (Figure 6-4).
SOFT TISSUE PATHOLOGY
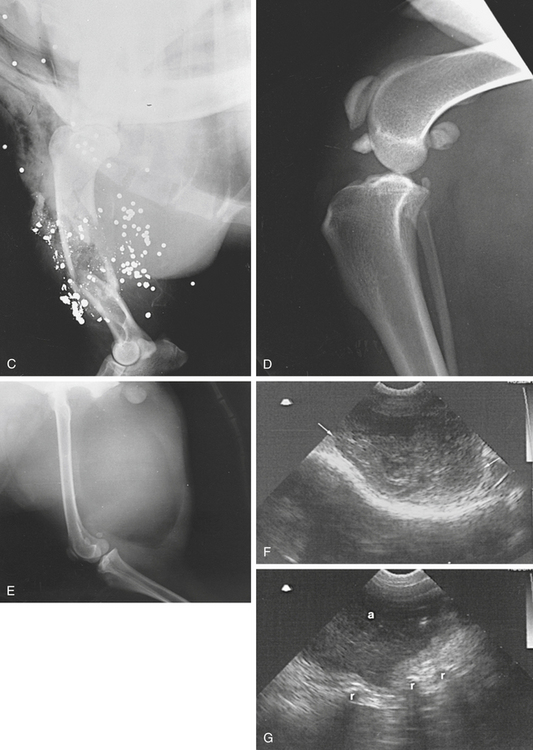
Swelling of soft tissue or soft tissue masses are frequently seen on radiographs. More detailed information is usually obtained by clinical examination. Emphysema is seen as gas shadows within the soft tissues or under the skin. Gas opacities are seen within the soft tissues after puncture of the skin, such as with a compound (open) fracture. Air shadows are seen within the soft tissues after surgery. Radiopaque foreign bodies in soft tissues are visible radiographically (Figure 6-5, A to E).
Soft tissue masses may be recognized because they displace adjacent structures. For example, a retropharyngeal mass will displace the larynx ventrally; a thyroid mass will displace the cervical trachea ventrally or laterally (see Figure 3-3, E). More specific details concerning soft tissue shadows are given in earlier chapters of this text.
Ultrasonography
Hematomas have a variable echogenic pattern, depending on the age of the lesion and the degree of clot retraction. Abscesses are predominantly anechoic, with floccules representing cellular debris. Focal hyperechoic areas may indicate the presence of free gas or mineralization.
Foreign bodies may be located in the soft tissues. Nonmetallic foreign bodies cause variable degrees of acoustic shadowing, whereas metallic foreign bodies are highly echogenic, causing large acoustic shadows and multiple reverberation artifacts. Failure to demonstrate a foreign body does not preclude its presence (see Figure 6-5, G).
THYROID GLAND
The thyroid gland lies caudal to the larynx and adjacent to the trachea. It is a paired structure that lies on either side of the trachea, and each part lies medial to the carotid artery. The two halves may be connected ventral to the trachea. It is not seen on plain radiographs until it becomes enlarged. An enlarged thyroid displaces the trachea in a variety of ways, depending on the location of the enlargement.
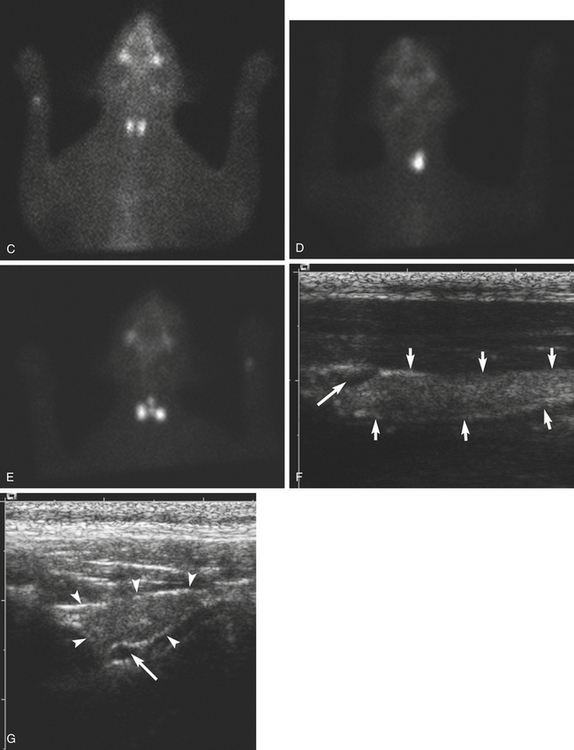
Ultrasonography
The thyroid gland is found by locating a carotid artery as a linear anechoic, pulsing structure deep to the jugular furrow. The transducer angle is approximately 45 degrees between the lateral and ventral aspects of the neck. The lobes lie medial to the carotid arteries and are fusiform, well-defined, homogeneous structures that are contained within the carotid sheath. They are isoechoic or hypoechoic with a granular echotexture. Each lobe is 2.5 to 3.0 cm long and 0.4 to 0.6 cm wide in dogs. In cats the length is about 2 cm, and the width is approximately 0.2 cm (Figure 6-6, A).