CHAPTER 5 The Pelvic Limb

PELVIS
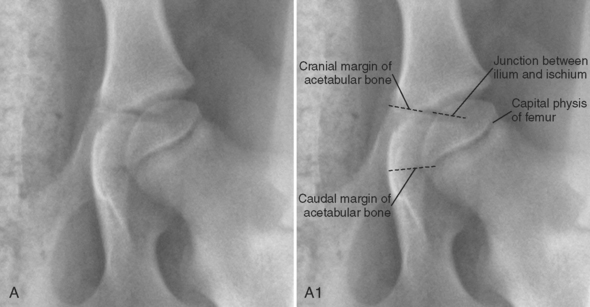
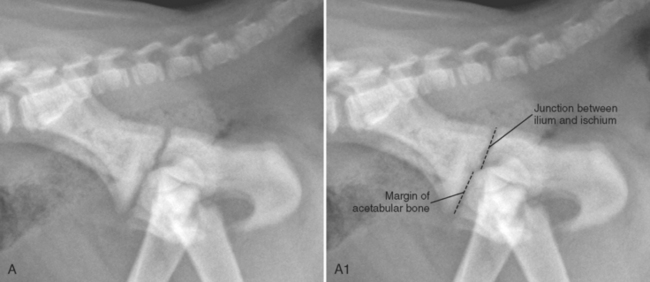
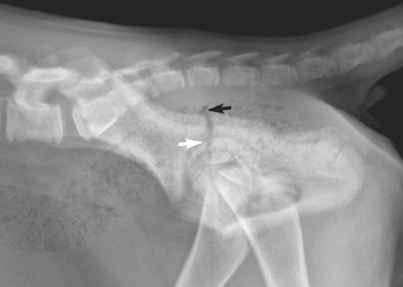
The pelvis is composed of four paired bones: ilium, ischium, pubic bone, and acetabular bone. The acetabular bone is a small triangular bone that lies between the caudoventral aspect of the ilium and the cranioventral aspect of the ischium (Figure 5-1). It fuses with adjacent bones at approximately 12 weeks of age to form the ventral portion of the acetabulum.1 Before fusion of the acetabular bone, there are many radiolucent junctions: between the cranial aspect of the acetabular bone and the ilium; between the caudal aspect of the acetabular bone and the ischium; and between the ilium and the ischium, dorsal to the acetabular bone (this junction is contiguous with the margins of the acetabular bone). Thus, superimposition of all of these radiolucent junctions makes it difficult to identify the acetabular bone in its entirety, although portions of it can be seen (Figure 5-2). Care should be taken to avoid misinterpreting the numerous cartilaginous junctions in the acetabular region of young animals as fractures (Figure 5-3). Superimposition of fecal material with the pelvis can also lead to an incorrect diagnosis of a pelvic fracture, especially in lateral radiographs (Figure 5-4).
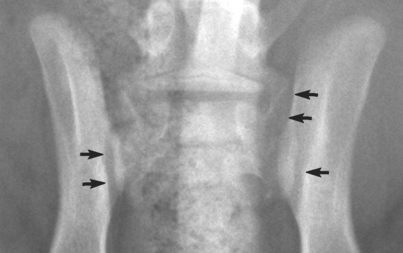
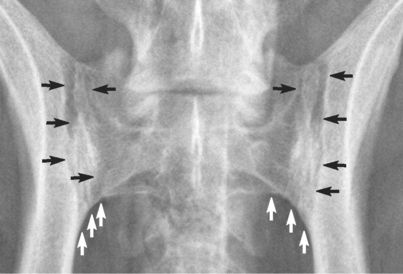
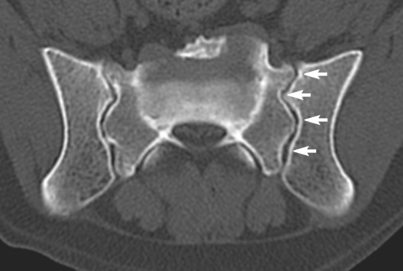
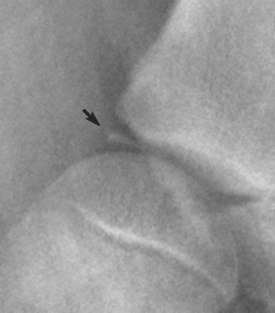
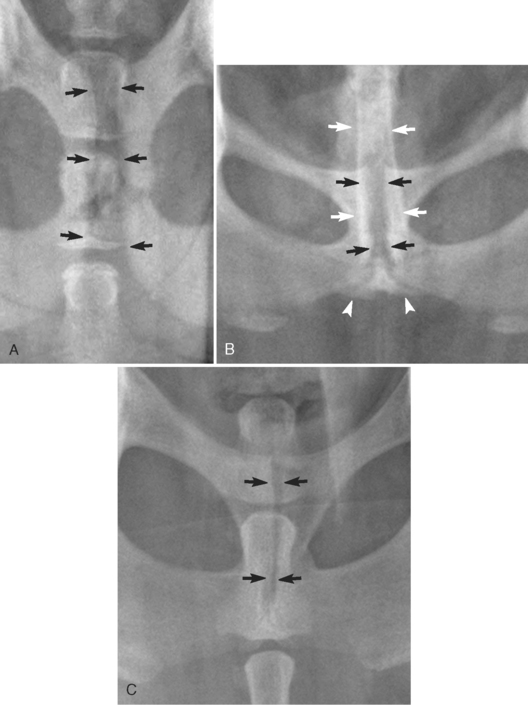
The ilium and the sacrum join at the sacroiliac joint, a combined synovial and cartilaginous joint that is united by a thin joint capsule. The union between the ilium and the sacrum is a synchondrosis.2 The cartilage between the ilium and the sacrum creates a radiolucent line separating the two structures. This radiolucency, which persists throughout life, can be confused with a sacroiliac fracture or subluxation in patients of all ages (Figures 5-5 and 5-6). In a ventrodorsal radiograph, the sacroiliac junction appears to be composed of multiple longitudinal radiolucent lines rather than a single line because the articulation is not perfectly opposing; interdigitations create alternating lines of opacity and lucency (Figure 5-7). The caudal margin of the normal sacroiliac joint is characterized by a smooth transition at the junction of the ilium and the sacrum (see Figure 5-6); the character of this transition is the key to detecting sacroiliac subluxation. If there is displacement of the ilium with respect to the sacrum, a malalignment, or step, will be formed at this transition.
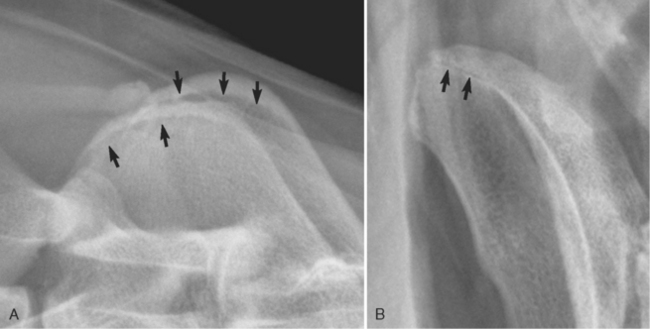
The ilium is divided subjectively into a cranially located wing, the most cranial portion of which is the iliac crest, and a caudally located body (Figure 5-8). The iliac crest is fused with the wing of the ilium in most dogs by 2 years of age, but a permanently incomplete fusion is common, occurring in more than 10% of dogs3 (Figure 5-9). This incomplete fusion can be misinterpreted easily as a fracture. Usually the nonfused iliac crest is seen in the lateral view; in the ventrodorsal view, the iliac crest is superimposed on the wing of the ilium and any incomplete union is typically not visible. However, if there is slight obliquity to the pelvis in the ventrodorsal view, the radiolucent junction between the iliac crest and wing of the ilium can occasionally be seen in that view as well (Figure 5-10).
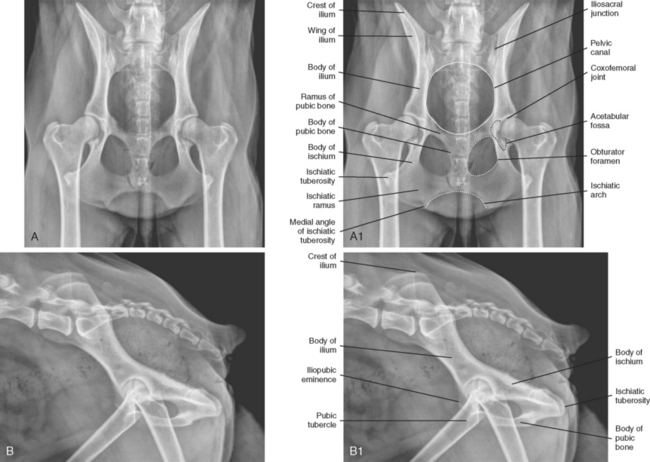

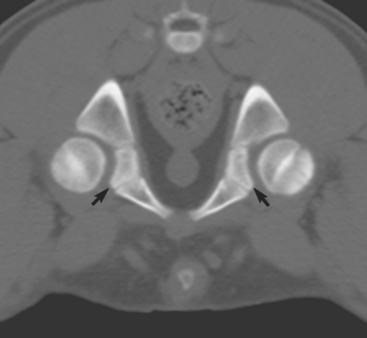
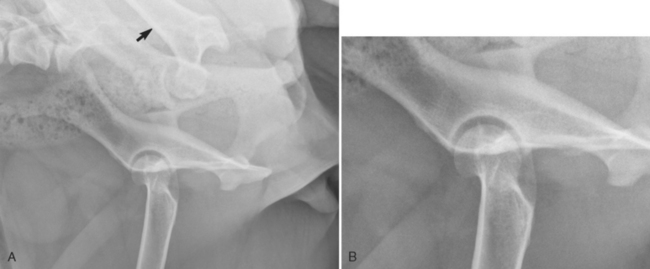
The acetabulum is formed at the confluence of the ilium, the ischium, and the pubis. It serves as a major articular component of the coxofemoral joint. The acetabulum is characterized by a depression, the acetabular fossa, that occupies the central portion of the articular surface in the ventrodorsal view (see Figure 5-8, A1, and 5-11). Congruency of the coxofemoral joint to characterize joint laxity is commonly assessed radiographically in the extended hip ventrodorsal view. Congruency should be evaluated cranial to the acetabular fossa (see the region of the white arrowheads in Figure 5-11). The acetabular fossa disrupts the smooth articulation between the femoral head and the acetabulum; thus congruency cannot be assessed in this area. In some young dogs, there is a small separate center of ossification located at the craniolateral margin of the acetabulum; this will eventually fuse with the ilium and should not be confused with a fracture fragment (Figure 5-12).

When the acetabulum is assessed, two additional views are sometimes used. One is the dorsal acetabular rim (DAR) view, which is a special view designed to assess the configuration of the dorsal acetabular rim. For the DAR view to be acquired, the anesthetized patient is placed in sternal recumbency and the pelvic limbs are pulled cranially. If correctly positioned with the x-ray beam centered on the pelvis, the x-ray beam will pass through the long axis of the ilial shaft and result in the superimposition of the wings of the ilium, the body of the ilium, the acetabulum, and the tuber ischii. This will result in an unobstructed projection of the dorsal rim of the acetabulum.4 In the DAR view of a normal dog, the lateral aspect of the coxofemoral joint space should be oriented horizontally, and the rim of the acetabulum should be relatively pointed (Figure 5-13). The second additional acetabular view is an open-leg lateral view of the acetabulum, which provides an oblique, unobstructed view of the acetabulum and the femoral head. To acquire this view, the subject is placed in lateral recumbency with the coxofemoral joint of interest positioned dependently, against the x-ray table. The nondependent leg is abducted laterally to the extent that its final position is actually dorsal to the dorsal aspect of the spine. The x-ray beam is then centered on the dependent hip joint of interest. The open-leg lateral view provides an unobstructed, slightly oblique view of the acetabulum and proximal femur (Figure 5-14).
The ischium, which is composed of a body, ramus, and tuberosity, contributes to the formation of the acetabulum, the obturator foramen, and the pubic symphysis (see Figure 5-8).1 The pubic symphysis is characterized by a fibrous union in most dogs younger than 5 years of age; after that time there is usually complete bony fusion.2 Before fusion, the relative radiolucency of the fibrous union of the pubic symphysis can be misinterpreted as a fracture (Figure 5-15). In male dogs, superimposition of fecal material, the caudal vertebrae, and the prepuce decreases the conspicuity of the pubic symphysis in many ventrodorsal radiographs by creating confusing summation opacities. The pubic symphysis is not visualized in lateral radiographs because the primary x-ray beam does not strike the junction in a parallel fashion in this projection.
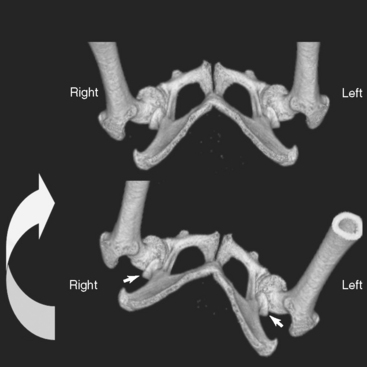
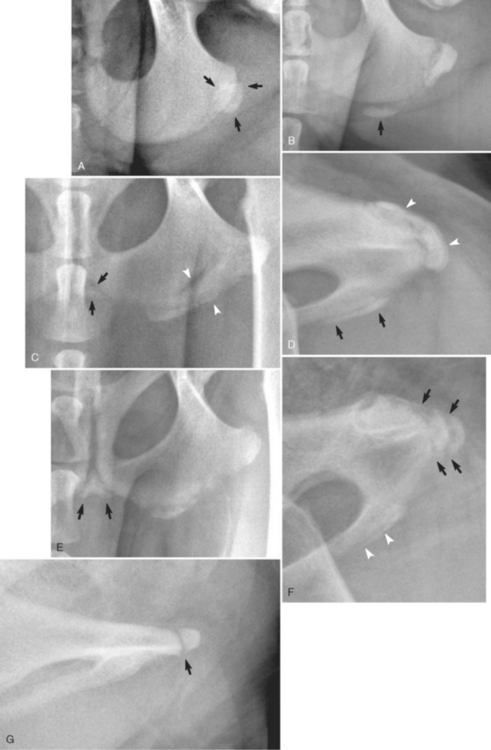
The caudal portion of the ischium, the ischiatic tuberosity, develops from a separate ossification center (Figure 5-16). Typically, ossification of the ischiatic tuberosity begins at the most lateral aspect of the ischium (see Figure 5-16, A). With age, the lateral aspect of the ossification center fuses with the ischium, and ossification of the cartilaginous tuber ischii continues medially (see Figure 5-16 B, C, and E). As ossification of the tuber ischii proceeds, some dogs will also develop a secondary center of ossification at the caudal aspect of the pubic symphysis, associated with the ischiatic arch (see Figures 5-15, C, and 5-16, C and E). In lateral radiographs of the pelvis, the secondary ossification centers of the caudal aspect of the pelvis are easily confused with fractures (see Figure 5-16, D, F, and G).
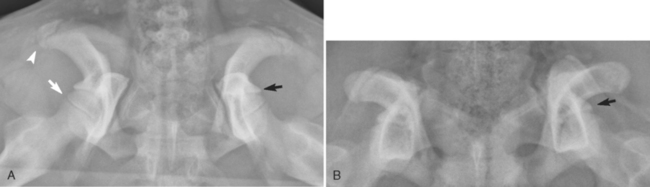
The pubic bone is composed of two rami and a body (see Figure 5-8). The pubic bone and the ischium bound the obturator foramen (see Figure 5-8). Assessing the symmetry of the obturator foramina in ventrodorsal radiographs is a good method to determine the degree of rotation of the pelvis that may have been present during radiography. Assessing the degree of rotation is important because rotation influences the apparent radiographic depth of the acetabulum and apparent radiographic congruity of the coxofemoral joint. With the dog in dorsal recumbency, the obturator foramina are not normally parallel with the dorsal plane; the plane of each foramen is angled from ventromedially to dorsolaterally. As a result, when the long axis of the body is rotated, the obturator foramen on the side opposite of the direction of rotation appears larger, and the coxofemoral joint on that side appears to have greater depth and congruency than the opposite coxofemoral joint (Figures 5-17 and 5-18). In addition, the iliac crest on the side of the direction of rotation appears wider because it is struck more en face by the primary x-ray beam (see Figure 5-18).