CHAPTER 1 Introduction
RADIOGRAPHIC TERMINOLOGY
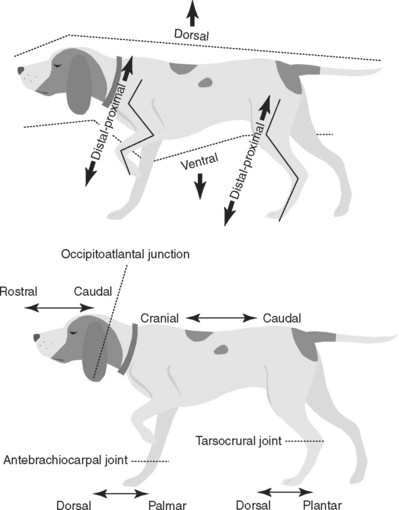
This book uses the standard method for naming radiographic projections approved by the American College of Veterinary Radiology (1). In general, this naming method is based on anatomic directional terms (as defined by the Nomina Anatomica Veterinaria) combined with the point-of-entrance to point-of-exit of the primary x-ray beam. Figure 1-1 diagrams the accepted anatomic directional terms. Several important concepts are commonly violated, leading to improper radiographic identification. In summary, these are:




VIEWING IMAGES
 Lateral views of any body part should be hung with the subject’s head, or the cranial or rostral aspect of the body part, facing to the examiner’s left.
Lateral views of any body part should be hung with the subject’s head, or the cranial or rostral aspect of the body part, facing to the examiner’s left.


STANDARD PROJECTIONS
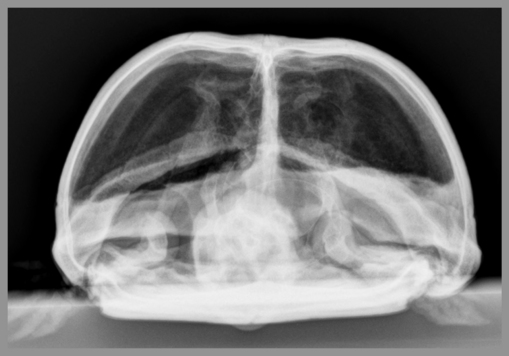
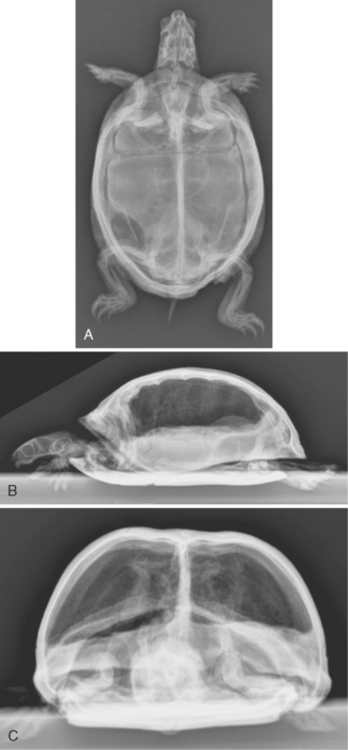
Most body parts being radiographed are usually subjected to multiple views at different beam angles. Most commonly, this involves views made at 90° to each other, termed orthogonal views. Table 1-1 lists the most common orthogonal views for the major body parts. It is critical to routinely make standard orthogonal views; the complexity of various anatomic parts is simplified by the repetitive aspect of looking at the same radiographic projections over and over. When an object is viewed in an unfamiliar orientation, relevant anatomy becomes less recognizable (Figure 1-2).
Table 1-1 Common Orthogonal Views for Major Body Parts
| Body Part | View | Orthogonal View |
|---|---|---|
| Skull | Lateral | Ventrodorsal or dorsoventral |
| Spine | Lateral | Ventrodorsal |
| Thorax | Lateral | Ventrodorsal or dorsoventral |
| Abdomen | Lateral | Ventrodorsal |
| Pelvis | Lateral | Ventrodorsal |
| Brachium, antebrachium, thigh, crus | Lateral | Craniocaudal or caudocranial |
| Manus | Lateral | Dorsopalmar |
| Pes | Lateral | Dorsoplantar |
OBLIQUE PROJECTIONS
This chapter presents examples of oblique radiography based on radiography of the canine tarsal and canine carpal joints.*
Dorsopalmar or Dorsoplantar View
The dorsopalmar or dorsoplantar view is one of the two basic orthogonal radiographic views of extremities. It is made when the x-ray beam strikes the dorsal (front) surface of a limb perpendicularly with the cassette or imaging plate behind the limb, perpendicular to the primary x-ray beam. The correct name of this view depends on whether the limb is a forelimb or hindlimb, and whether the central portion of the primary x-ray beam is proximal or distal to the antebrachiocarpal or tarsocrural joints (Table 1-2).
Table 1-2 Correct Names for Radiographic Projections of a Limb Where the X-Ray Beam Strikes the Front Surface of the Limb and the Cassette or Imaging Plate Is Directly Behind the Limb
| Correct Name of View | Orientation |
|---|---|
| Dorsopalmar | Primary x-ray beam strikes front surface of forelimb at antebrachiocarpal joint or distal. Cassette or imaging plate is perpendicular to primary x-ray beam. |
| Dorsoplantar | Primary x-ray beam strikes front surface of hindlimb at tarsocrural joint or distal. Cassette or imaging plate is perpendicular to primary x-ray beam. |
| Craniocaudal | Primary x-ray beam strikes front surface of forelimb or hindlimb proximal to antebrachiocarpal joint or tarsocrural joint. Cassette or imaging plate is perpendicular to primary x-ray beam. |
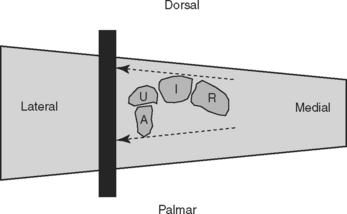
In a dorsopalmar view of a carpus, for example, the x-ray beam strikes the dorsal surface of the carpus with the image plate behind the carpus oriented perpendicular to the primary x-ray beam (Figure 1-3). In this geometric arrangement, only the medial and lateral aspects of the structure of interest can be visualized in an unobstructed manner (see Figures 1-3 and 1-4). This does not mean that only the edges of the structure can be evaluated; the infrastructure can be assessed but the lateral and medial surfaces are primarily where a periosteal reaction or cortical erosion can be identified.
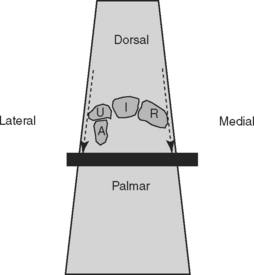

Figure 1-4 The left panel shows a dorsoplantar radiograph of a canine tarsus. The middle panel shows a threedimensional rendering of a normal right canine tarsus as seen from the perspective of the x-ray beam when making a dorsoplantar radiograph. The right panel shows a threedimensional rendering of a normal right canine tarsus, also as seen from the perspective of the x-ray beam when making a dorsoplantar radiograph, but where each bone has been colorized (see Color Plate 1). The colorized version makes it easier to comprehend the extent of overlap. Note in the radiograph how the only aspects of the tarsal bones that are projected in an unobstructed fashion where the surface can be evaluated are the medial and lateral aspects of the tarsus.
Lateral View
The complementary orthogonal view to the dorsopalmar (or dorsoplantar) view of the extremities is the lateral view. It is made when the x-ray beam strikes the side surface of a limb with the cassette or imaging plate on the opposite side of the limb, perpendicular to the primary x-ray beam (Figure 1-5). These views are most often referred to as lateral views, although lateromedial or mediolateral is more correct depending on whether the lateral or medial aspect of the limb, respectively, is struck by the primary x-ray beam.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


