CHAPTER 7 The Abdomen
Standard radiographic views of the abdomen include a lateral view and a ventrodorsal (VD) view; dorsoventral (DV) views of the abdomen are rarely made and are not described herein. In general, abdominal radiographs should be made without fasting or enema administration. This way the image represents the natural condition of the patient and avoids the alteration of normal bowel content patterns that would result from an enema. In addition, the gastric contents are sometimes relevant in terms of making the correct diagnosis. All figures in this chapter are of patients for which no special preparation was undertaken prior to radiography. The instances in which preparation for abdominal radiography is needed is beyond the scope of this work.
Pulling the pelvic limbs caudally during radiography can complicate interpretation. In the VD view, pulling the pelvic limbs caudally leads to skin folds, which create linear opacities that can interfere with assessment of the caudal aspect of the abdomen. It is preferable to flex the pelvic limbs for the VD radiograph so that the caudal aspect of the abdominal wall is not taut but is relaxed with greater lateral expansion and less crowding (Figure 7-1). In lateral view, femurs should be approximately perpendicular to the lumbar spine and neither pushed cranially nor pulled caudally.

Radiographic visualization of abdominal organs requires that there be adequate normal surrounding fat to provide contrast. This is true for the intraperitoneal and retroperitoneal spaces. Fat provides contrast to abdominal organs because it is of lower physical density and lower effective atomic number (Figure 7-2). Fat mainly provides enhanced visualization of the periphery of organs; the character of the interior of abdominal organs relates to their constituency. Most abdominal organs are of soft tissue opacity, but the lumen of the gastrointestinal tract commonly contains material that is either more radiopaque than soft tissue, such as bone fragments, or less radiopaque than soft tissue, such as gas. The homogeneity and radiographic opacity of the intraperitoneal fat and retroperitoneal fat should be similar. Discrepancies between the opacity of fat in these two compartments can indicate the presence of retroperitoneal or intraperitoneal disease.1
A relative lack of fat in the abdomen, as seen in emaciated animals, reduces the conspicuity of the margins of abdominal organs (Figure 7-3). Serosal margin conspicuity is also reduced in very young patients, likely due to a relatively reduced volume of abdominal fat (Figure 7-4). It has been theorized that peritoneal fat in young patients may be more hydrated than fat in adults, thus increasing its opacity and decreasing its ability to provide radiographic contrast.2
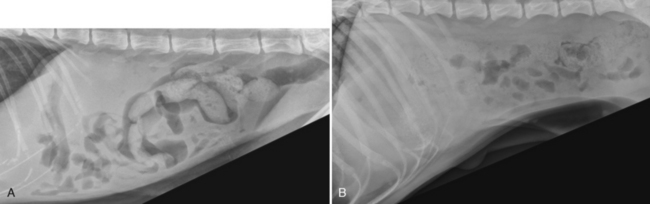
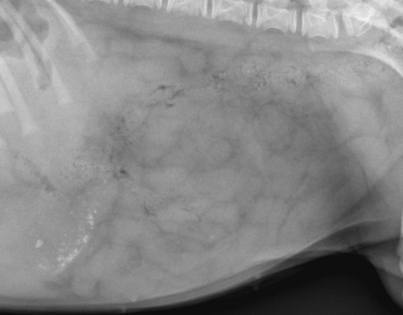
Figure 7-4 Lateral radiograph of an 11-week-old golden retriever. Conspicuity of serosal margin detail is diminished due to the relative lack of abdominal fat; this is a common finding in young animals. Margin visualization is, however, better than in patients that are undernourished and emaciated (compare with Figure 7-3).
Cats, particularly those in a state of positive caloric balance, can accumulate massive amounts of intraperitoneal and retroperitoneal fat. The largest collections of abdominal fat in cats are in the retroperitoneal space and in the cranioventral aspect of the abdomen. Fat accumulation in the cranioventral aspect of the abdomen, some of which is in the falciform ligament, can create a large mass effect in this region (Figure 7-5). The falciform ligament is formed by the two layers of the ventral aspect of the mesogastrum, thus fat in the falciform ligament is actually extraperitoneal.3 Falciform fat is commonly misinterpreted as peritoneal effusion by inexperiencd interpreters; basic principles of radiographic opacity dictate this cannot be true or there would be border effacement of the liver margin and loss of serosal margin detail.
LIVER
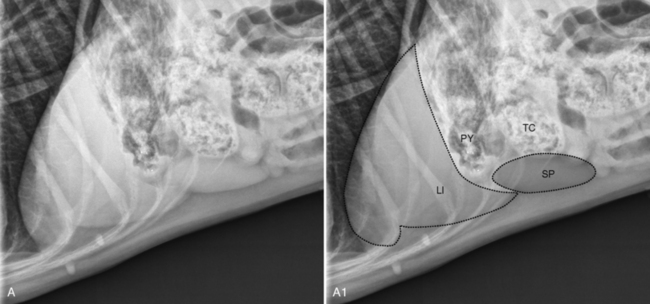
The liver is located in the cranial aspect of the abdomen, between the diaphragm and stomach. Most of the visible liver mass is to the right of midline (Figure 7-6). The liver should be of homogeneous soft tissue opacity.
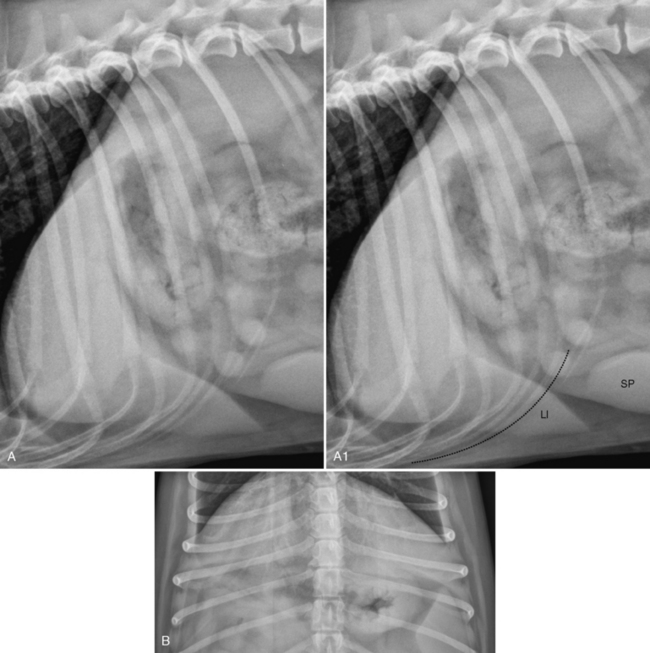
There is individual variation in the size of the normal liver in the dog and the cat, making the distinction between a mildly enlarged or mildly small liver from a normal liver highly subjective and relatively inaccurate. The position of the stomach is one parameter that is commonly used as an indicator of liver size. It is generally accepted that if the liver is normal, a line connecting the gastric fundus with the gastric pylorus in a lateral radiograph, termed the gastric axis, will range between being perpendicular to the spine or angled such that the gastric axis is parallel with the intercostal spaces (see Figure 7-6, A1). If the gastric axis extends outside of this range, cranially or caudally, then the possibility that the liver is decreased or increased in size, respectively, should be considered. It is important to note that the accepted normal range of the gastric axis in lateral radiographs is only a guideline, and slight deviation in the position of the gastric axis outside of the accepted normal range can be encountered when there is no pathologic liver abnormality.
Another commonly used criterion for liver size in lateral radiographs is extension of the liver beyond the costal arch (the costal arch is formed by the border of the last few costal cartilages). However, the costal arch is not a precise demarcation between a normal liver and an enlarged liver, and it cannot be used as a definitive landmark to assess liver size. It is important to recognize that a normal liver can extend beyond the costal arch (Figure 7-7). Unfortunately, the cutoff point between a normal size liver and an enlarged liver based on extension beyond the costal arch is vague.
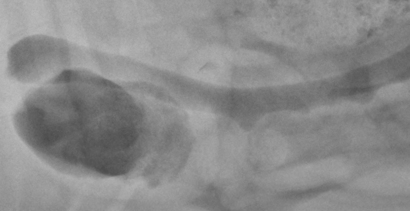
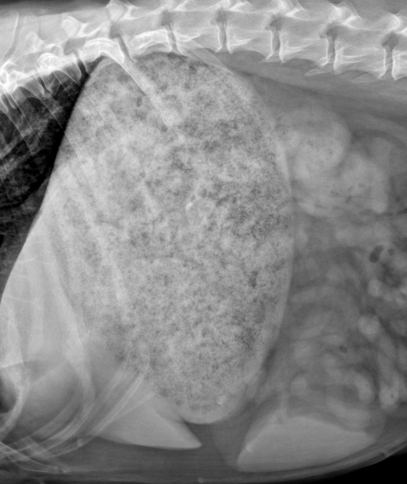
Another situation in which a normal liver might extend beyond the costal arch is a distended stomach placing pressure on the liver and causing its ventral aspect to slide caudally beyond the costal arch (Figure 7-8).
A change in shape to the margin of the portion of the liver that extends caudal to the costal arch from a gradual taper (see Figures 7-6, A, and 7-7, A) to a more rounded configuration is another finding often associated with liver enlargement.
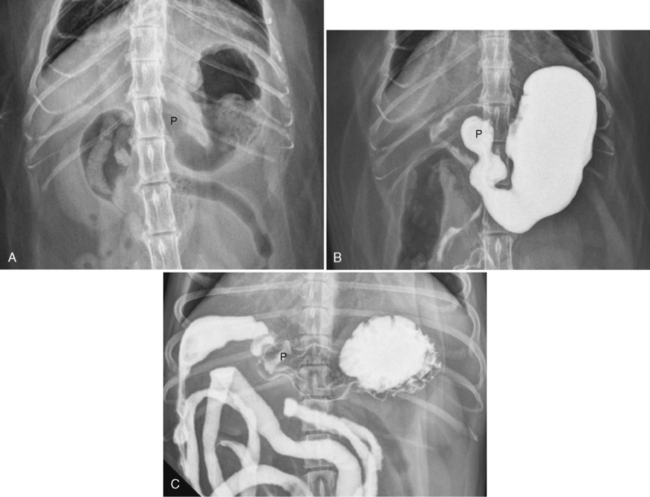
The criteria for evaluating liver size in cats are the same as in dogs. However, it is important to recognize that the gastric pylorus in cats is normally located more medially than in dogs, residing nearly on the midline. Thus, the position of the gastric pylorus is rarely used to assess liver size in VD abdominal radiographs in cats (Figure 7-9).
The gallbladder is situated between the quadrate lobe medially and the right medial lobe laterally, in the cranioventral aspect of the liver. In most patients, the normal gallbladder is not seen radiographically. Occasionally, especially in cats, a round opacity is superimposed on the ventral aspect of the liver or extends slightly beyond the margin of the ventral aspect of the liver. This round opacity can be is created by a normal, but modestly distended, gallbladder (Figure 7-10). This can be seen when there is no associated evidence of liver or gallbladder disease. However, visualization of this opacity is not always a normal finding and, if clinically indicated, the liver should be assessed using other methods.
SPLEEN
The spleen, a lymphatic organ, is located in the left hemiabdomen. The spleen should be of homogeneous soft tissue opacity. The proximal aspect of the spleen, commonly referred to as the head of the spleen, is located in close approximation to the gastric fundus. It is held loosely in this position by the gastrosplenic ligament and the short gastric arteries and veins that communicate with the splenic vessels.4 These short gastric arteries and veins can be less well-developed in the cat.5 The distal extremity of the spleen, commonly called the tail of the spleen, is more mobile and variable in position than the proximal extremity.
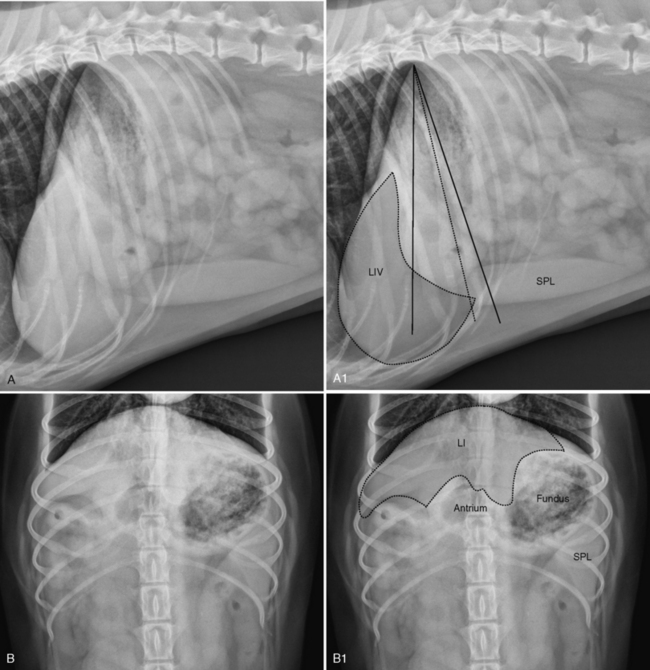
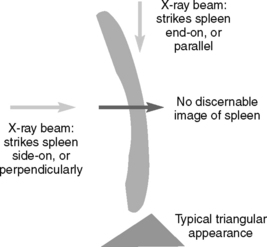
When the spleen is visualized radiographically, it is important to realize that the entire spleen is not seen in a single radiographic view. When the x-ray beam is oriented along or parallel to (called end-on projection) a length of the spleen, it typically has a triangular shape. If the body of the spleen is struck perpendicularly by the primary x-ray beam (called side-on projection), there usually is insufficient absorption of the x-rays to see that portion of the spleen (Figure 7-11). Sometimes, portions of the spleen proximal and distal to a region struck end-on by the x-ray beam also absorb sufficient x-rays to be conspicuous. The extent of the spleen that can be seen depends on the thickness of the spleen, its orientation to the primary x-ray beam, and the contrast resolution of the imaging system.
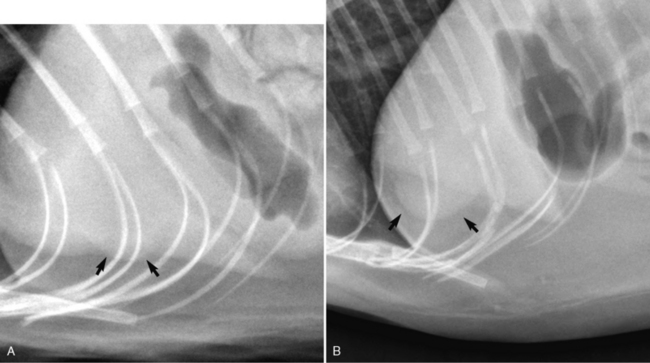
In lateral abdominal radiographs of the dog, the distal extremity of the spleen is the portion seen most commonly (Figure 7-12, A-B). In lateral recumbency, the distal extremity lying adjacent to the ventral abdominal wall is oriented end-on to the primary x-ray beam. Occasionally, as mentioned previously, the portions of the spleen extending peripherally from the distal extremity can also be seen (see Figure 7-12, A1 and B1; white arrows).
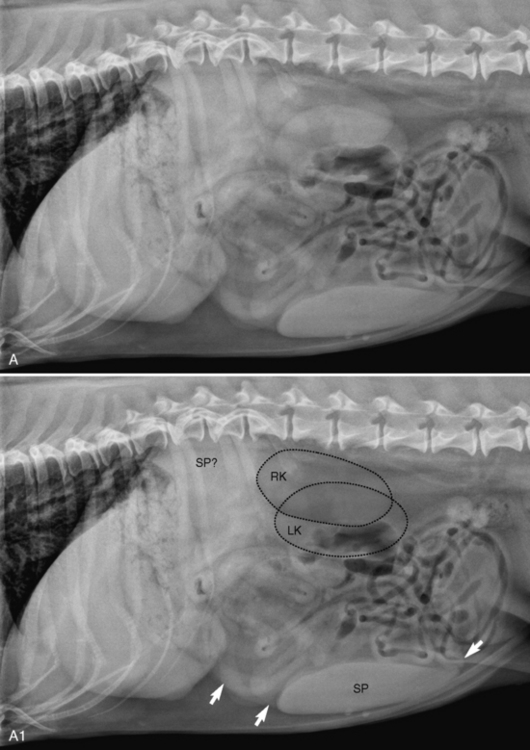
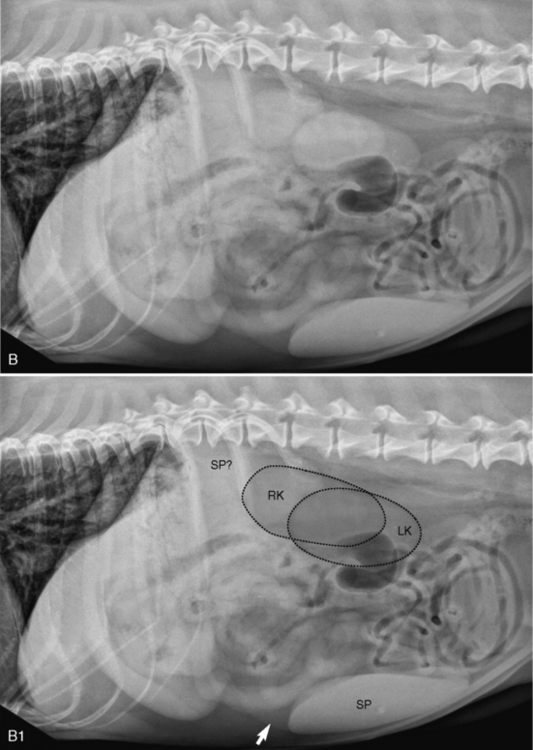
With a moderately sized normal spleen, the proximal portion might be oriented in a way that creates an ill-defined mass effect in lateral radiographs in the region between the gastric fundus and the kidneys, without being visualized as a distinct triangular structure (see Figure 7-12, A1 and B1). Other imaging modalities would be needed to interpret this finding correctly, because a mass effect between the gastric fundus and kidneys in lateral radiographs could represent an abnormal mass.
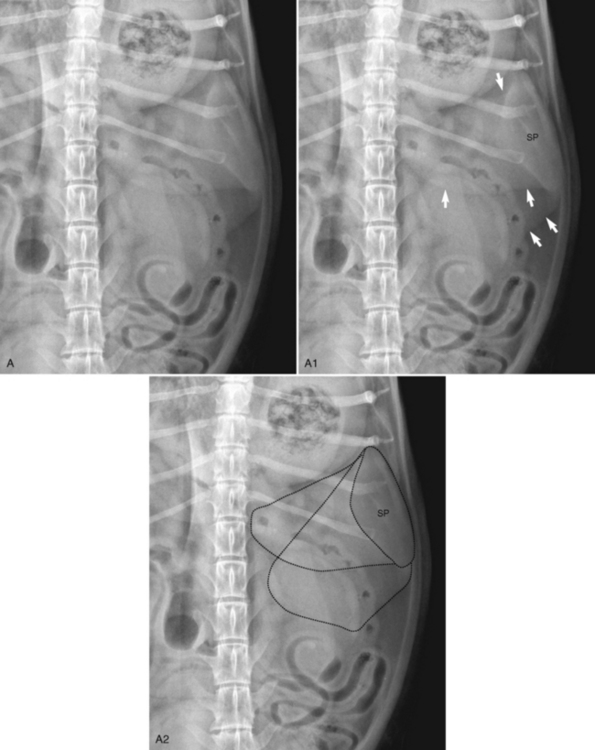
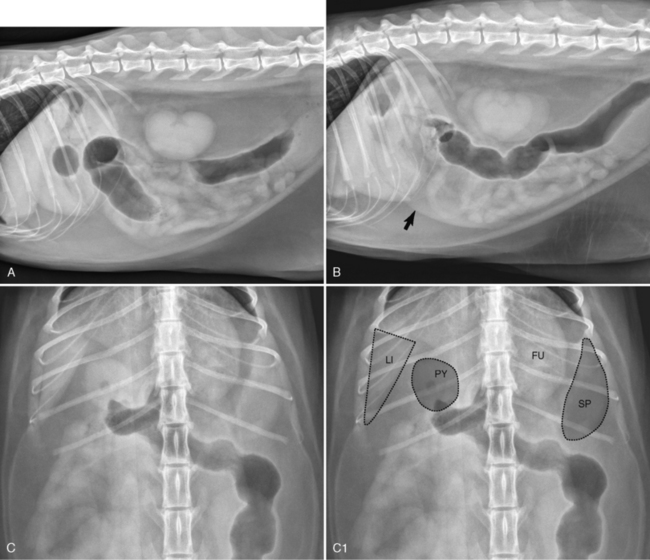
In VD abdominal radiographs of the dog, it is the proximal extremity of the spleen that typically is seen (Figure 7-13). Again, this is due to the portion of the proximal extremity lying adjacent to the left abdominal wall being oriented end-on to the primary x-ray beam. Similar to lateral views, portions of the spleen extending peripherally from the proximal extremity can sometimes be seen (see Figure 7-13).
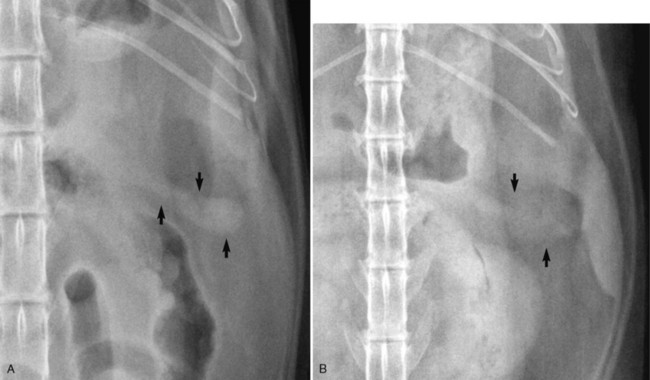
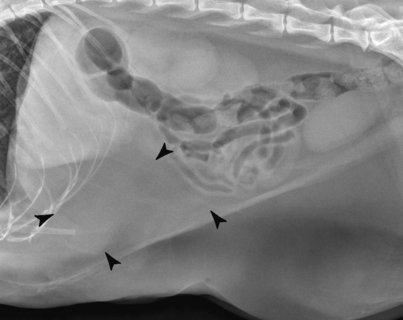
In the dog, due to its mobility, the distal extremity of the spleen can be located in the cranioventral aspect of the abdomen and can create an oblong opacity that is often misdiagnosed as an enlarged liver lobe (Figure 7-14). The key to correctly distinguishing between spleen and liver in this circumstance relates to the location of the cranial aspect of the suspicious opacity. If the opacity is the distal extremity of the spleen, its cranial margin will not extend cranial to the gastric pylorus and there will be a plane of fat opacity between it and the liver (see Figure 7-14), except in emaciated subjects. If the suspicious opacity is an enlarged liver lobe, the opacity can be traced cranial to the gastric pylorus and there will not be a plane of fat opacity between it and the liver.
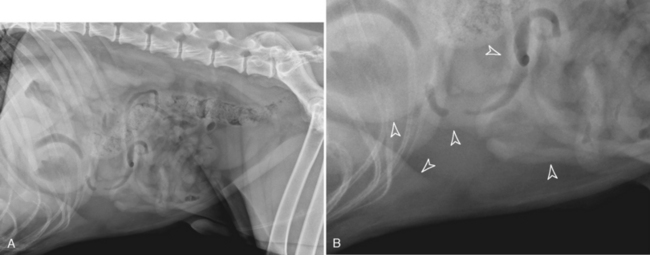
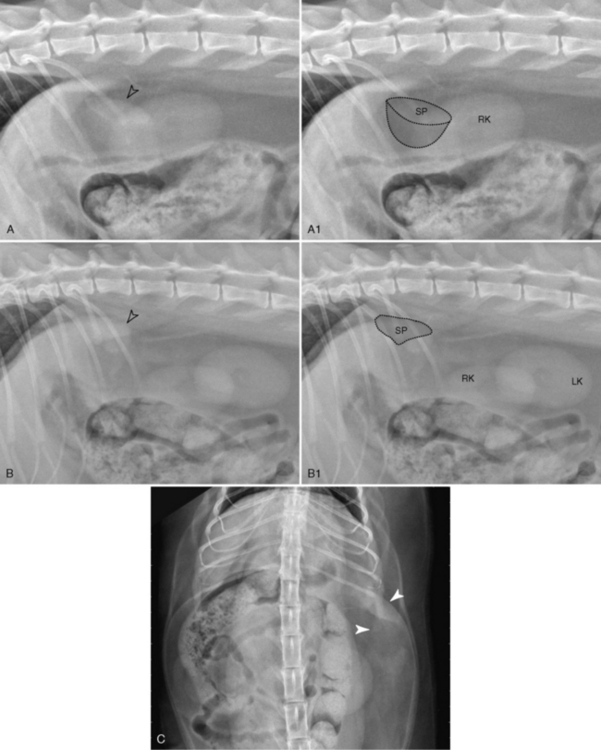
As noted previously, the distal extremity of the spleen is rarely seen in lateral radiographs in cats. The most common appearance of a normal spleen in the cat is visualization of the spleen in the VD view, lateral to the gastric fundus, with the spleen not being seen in either a left or right lateral view (Figure 7-15). Occasionally in cats with abundant peritoneal fat, the proximal extremity of the spleen can be seen in lateral radiographs just caudal to the stomach (Figure 7-16). This appearance can be confused with an adrenal mass; if there is any question of the identity of a radiographic opacity caudal to the stomach in the cat, more specific imaging modalities of the region should be used.
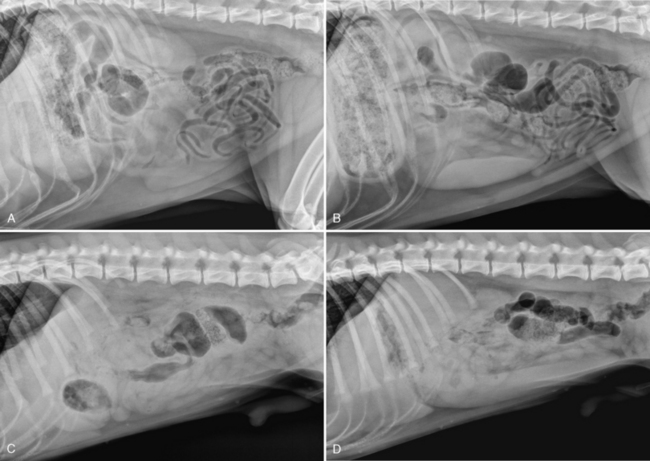
The great mobility of the spleen results in it having a different appearance in left versus right lateral radiographs of the abdomen and, although the exact changes in splenic position that occur as a function of recumbency have not been completely characterized, the distal extremity seems to be more conspicuous in right lateral radiographs (Figure 7-17). The effect of spleen conspicuity as a function of recumbency is most likely due to compression of the dependent portion of the abdomen leading to a change in the location of the spleen.
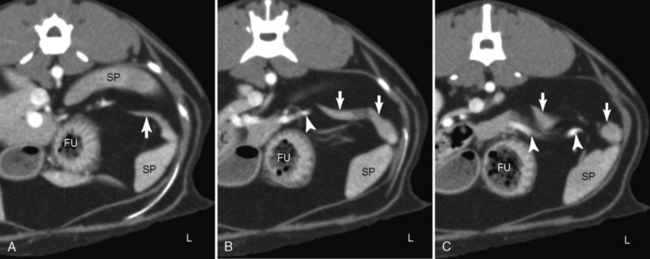
PANCREAS
The normal pancreas is not visible radiographically in the dog. In the cat, the left lobe of the pancreas extends lateral to the level of the gastric fundus and, in this location, is not in contact with any other soft tissue organ (Figure 7-18). If there is adequate fat surrounding the left lobe, it can be identified in VD abdominal radiographs as a fusiform opacity medial to the midportion of the spleen (Figure 7-19).