CHAPTER 8 The Oropharynx and Tonsils
NORMAL FINDINGS
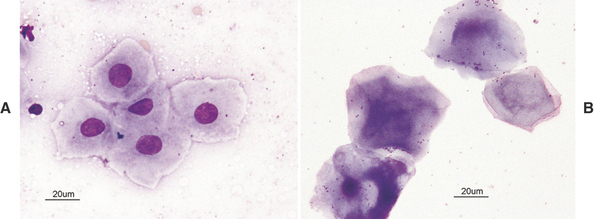
In order to correctly identify abnormal criteria, recognition of normal findings is essential. The oropharynx and tonsils are covered by mature squamous epithelial cells (Figure 8-1). These are large, flat, and round to slightly angular. They have abundant pale cytoplasm and small round nuclei that exhibit condensed chromatin. Nucleoli are not visible and some cells are anuclear. The presence of occasional intermediate squamous cells with slightly larger, less condensed nuclei is normal (Figure 8-2).
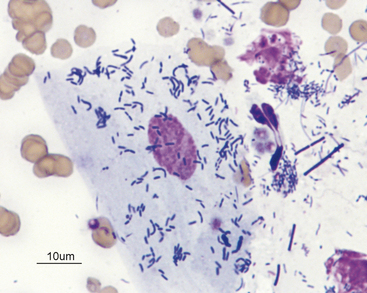
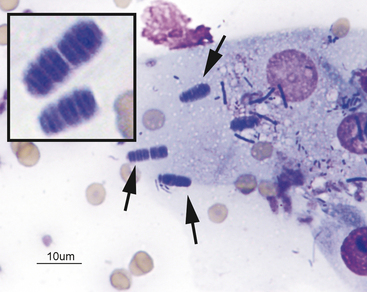
The normal squamous cells frequently exhibit a mixed bacterial population adhered to their surfaces (Figure 8-3). These bacteria are also usually present in the background between cells. The normal flora includes aerobic and anaerobic bacterial rods and cocci. Observation of spirochetes is considered normal. Yeast are never considered to be normal. One bacterium, Simonsiella spp., has a characteristic palisading appearance and is a normal inhabitant of the oropharynx (Figure 8-4). It should never be mistaken for a pathogen. If the bacterial population is dominated by only one type of bacteria, that would be considered abnormal.
THE OROPHARYNX
Nonneoplastic Lesions
Inflammation
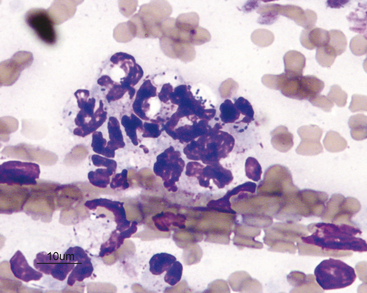
Infectious agents can be observed; however, their absence from a sample does not rule out the possibility of an infectious etiology. If the inflammatory lesion is caused by a primary bacterial infection or complicated by secondary bacterial infection, a homogenous population of bacteria is often seen and many will be phagocytized within neutrophils (Figure 8-5).
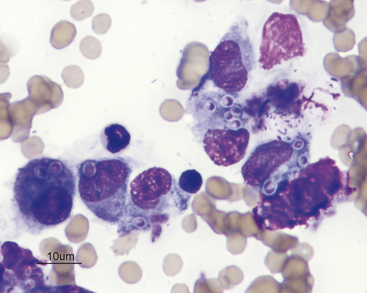
If the lesion is granulomatous, such as from a foreign body or yeast/fungal infection, a more evenly mixed population of neutrophils, macrophages, lymphocytes, and plasma cells is observed, with variable numbers of fibrocytes and fibroblasts that are indicative of physiologic fibroplasia (Figure 8-6). In some areas of the country, histoplasmosis in cats can present with oral lesions as the predominant physical examination finding. In these cases, a diagnosis can be made based on identification of organisms from proliferative oral lesions.
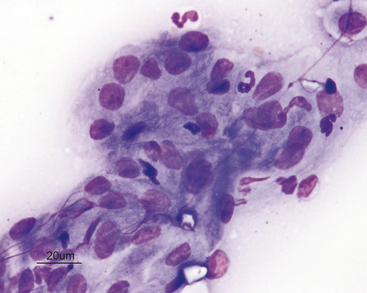
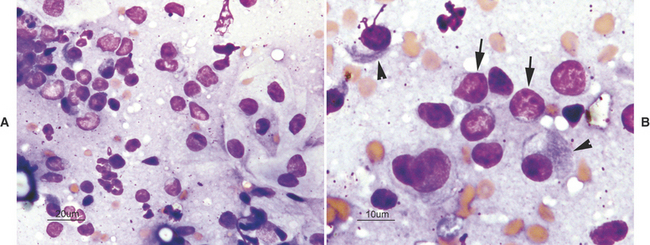
An inflammatory infiltrate characterized by a predominance of mature lymphocytes and plasma cells with scattered other inflammatory cells is seen in samples from cats with chronic gingivitis/stomatitis (i.e., lymphocytic-plasmacytic gingivitis/stomatitis). The characteristic inflammatory cells are typically admixed with normal or dysplastic epithelial cells (Figure 8-7).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


