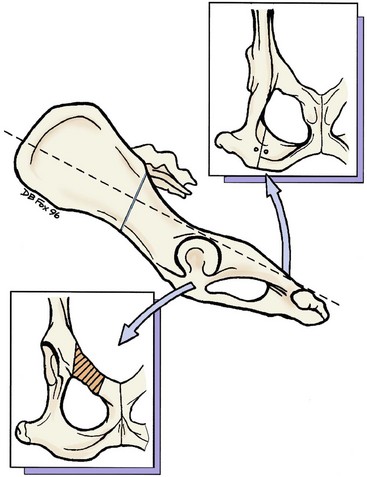
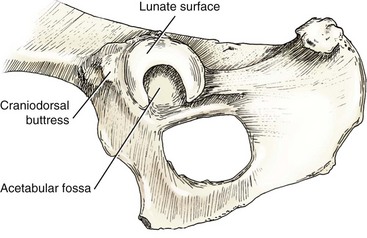
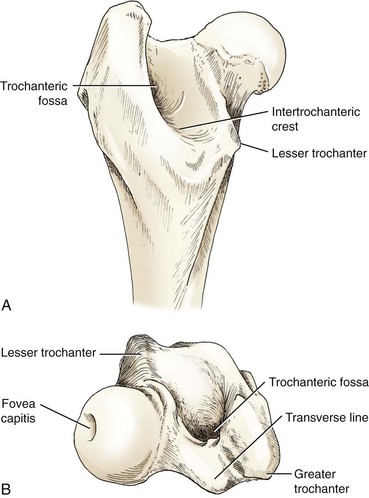
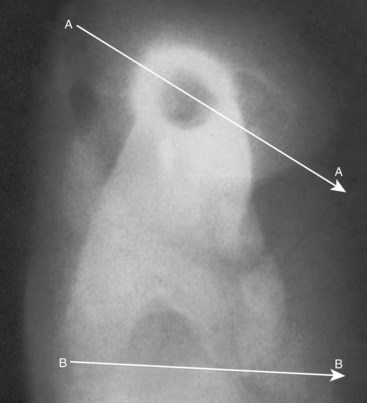
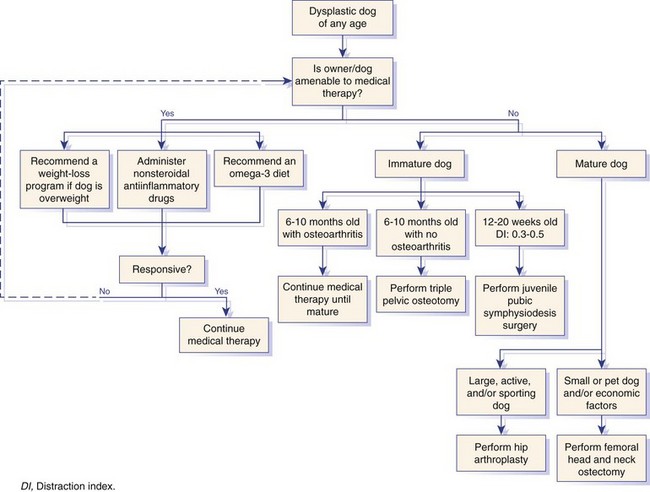
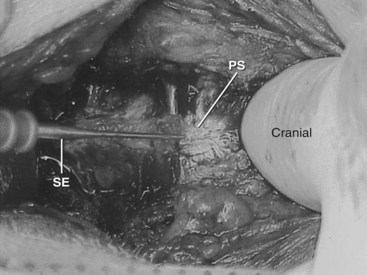
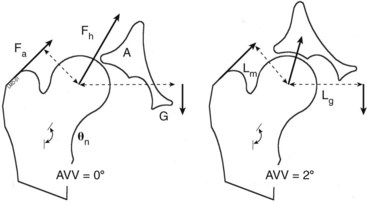
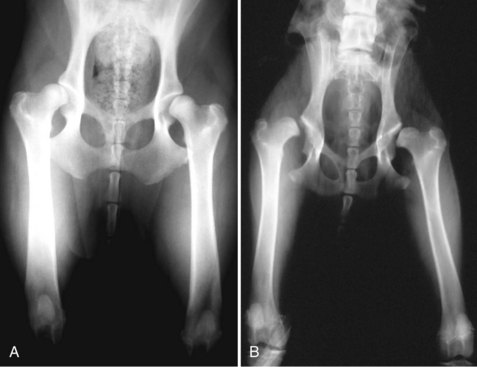
Chapter 60 The canine pelvis is composed of the paired os coxae (or hip bone), the sacrum, and the first caudal vertebrae. Each os coxae is developmentally composed of the ilium, ischium, pubis, and acetabular bones, which fuse at 12 weeks of age in the dog.37 The canine acetabulum, composed of the fusion of ilium, pubis, ischium, and acetabular bones, is a deep cavity bounded dorsally, cranially, and caudally by the acetabular rim and surfaced in those areas with articular cartilage. These dorsal, cranial, and caudal surfaces are also known as the lunate surfaces of the acetabulum. Medially and ventrally, the acetabulum is indented by a notch, the acetabular notch. The cranial and caudal surfaces of the acetabular notch are bridged by the transverse acetabular ligament, which continues around the remainder of the acetabulum as the labrum. The nonarticular, thin, depressed medial area lateral to the notch and extending to the lunate surface is the acetabular fossa (Figure 60-1), which contains the origin of the ligament of the head of the femur. The acetabulum is normally directed slightly caudally in relation to the midline of the hemipelvis in a position referred to as acetabular retroversion. Placement of acetabular prostheses in a mildly retroverted position is important for optimal total hip arthroplasty. Placement of a prosthesis with an iatrogenic cranially directed fossa is referred to as acetabular anteversion and predisposes to hip joint luxation. A neutral or straight lateral position of the acetabulum is known as acetabular normoversion. The proximal canine femur is composed of the femoral head and neck and the greater, lesser, and third trochanters (Figure 60-2). The hemispherical femoral head is covered over its entire surface with articular cartilage, with the exception of a small depressed area on the medial head, the fovea capitis femoris, which serves as the insertion of the ligament of the head of the femur. The femoral neck is normally directed slightly cranial, or anteverted, to the femoral diaphysis (also known as a positive angle of femoral torsion), and this cranial orientation is important for understanding positioning for femoral stem prostheses (Figure 60-3). The normal angle of femoral anteversion is approximately 27 degrees and ranges from 12 to 40 degrees; a negative angle of femoral torsion is known as retroversion, and a neutral or zero angle is referred to as normoversion. Retroversion of the femoral component during total hip arthroplasty may predispose to hip joint luxation. Between the femoral neck and the greater trochanter is the trochanteric fossa. The greater trochanter is the insertion point of the middle and deep gluteal and piriformis muscles, the lesser trochanter is the insertion point of the iliopsoas muscle, and the third trochanter is the insertion site of the superficial gluteal muscle. Distally, the body of the femur is a cylindrical shaft of bone with few muscular attachments except for the vastus intermedius muscle, which inserts on the caudal, roughened linea aspera. The femoral diaphysis has a slight craniocaudal bow, which can affect placement of the femoral prosthesis in total hip arthroplasty. Canine hip dysplasia has been portrayed historically as a biphasic clinical syndrome that is manifested by differing clinical signs at different ages. However, canine hip dysplasia is more accurately a monophasic and linear progression of osteoarthritis that we choose to classify in a biphasic mode for discussion of pathogenesis and diagnosis, because of the indications for current surgical treatment options (see Chapter 59). Clinical signs in skeletally immature dogs are due primarily to the pain of hip laxity, but clinical signs in skeletally mature dogs commonly are related to joint remodeling, loss of joint mobility, and the discomfort of osteoarthritis. The surgical options recommended for each dog should and do differ, depending on the age of the animal (Figure 60-4). Medical and physical rehabilitation therapies are applicable to dogs of any age. Medical therapy for hip dysplasia commonly comprises some combination of weight loss, nonsteroidal antiinflammatory drugs, and dietary changes such as the addition of omega-3 fatty acids. The effects of weight loss on improvement of clinical signs in dysplastic dogs of any age cannot be underestimated.77,83 Likewise, dietary supplementation with omega-3 fatty acids has been shown to decrease joint inflammation, improve peak vertical force during ground reaction force analysis, and improve clinical outcome as assessed by veterinarians and clients.108,109 Surgically induced premature closure of the pubic symphysis has been shown to cause mediolateral shortening of the cranial pubic rami.80,127 Shortened pubic bones, fixed to the ventromedial aspect of the acetabulum, cause rotation of the acetabula ventrally, or ventroversion, during growth of the pelvis, and thus create increased coverage of the femoral head by the acetabulum. The procedure results in acetabular ventroversion and decreases hip distraction indices, pelvic inlet circumference, and pelvic width in treated dogs compared with control dogs.127 The effect is similar to the rotation gained by a triple pelvic osteotomy without the greater expense, pain, and recovery associated with triple pelvic osteotomy. The procedure is effective if proper consideration is given to the age of the dog, the degree of laxity, and other selection criteria. The incidence of osteoarthritis was dramatically decreased at 2 years of age in dysplastic dogs on which juvenile pubic symphysiodesis had been performed at 15 or 20 weeks of age.90 A prospective clinical study compared long-term outcomes of dysplastic dogs undergoing juvenile pubic symphysiodesis with outcomes from triple pelvic osteotomy.74 No significant differences were noted in lameness scores, extension of the hip joint, distraction index, peak vertical force, acetabular angle, radiographic osteoarthritis score, or owner-assigned clinical function scores between treatments, although the dorsal acetabular rim angle was significantly greater in dogs that underwent juvenile pubic symphysiodesis. This procedure does not eliminate joint laxity or progression of osteoarthritis in dysplastic dogs.74 In a prospective study of 217 puppies 14 to 22 weeks of age treated with juvenile pubic symphysiodesis or no surgery, juvenile pubic symphysiodesis increased the odds of limiting the progression of hip dysplasia in puppies with mild to moderate laxity, although it was less effective if the puppies were severely affected.133 Pubic symphysiodesis was ineffective in dogs older than 22 weeks of age. The procedure is indicated primarily for puppies 12 to 20 weeks of age with palpable hip joint laxity. Distraction index radiography is a reliable method to determine hip joint laxity in dogs 4 months of age and older.2,125 Juvenile pubic symphysiodesis is more effective if done in younger puppies, particularly in puppies younger than 18 weeks of age.8,90 A 10 to 15 degree per hip improvement is expected if performed at 16 weeks of age, but minimal improvement is seen when the procedure is performed at 20 to 22 weeks. Screening of puppies at risk at 16 weeks of age is recommended. Identification of puppies that will benefit from juvenile pubic symphysiodesis is challenging. Puppies with mild to moderate palpable laxity and radiographic evidence of a predisposition (laxity, joint incongruency) are the best candidates for juvenile pubic symphysiodesis.134 Puppies with severe laxity and severe joint incongruency often demonstrate continued progression of disease despite the surgical procedure.134 No studies have been performed to identify and validate definite selection criteria for juvenile pubic symphysiodesis. It is known that increasing laxity, as measured by the distraction index, is associated with increased risk of developing radiographic osteoarthritis of the hip joint, and that this relationship is breed specific. However, in general, dogs with a distraction index of less than 0.3 do not develop radiographic osteoarthritis, and risk increases as the distraction index increases. Disease-susceptibility curves indicate a sigmoidal relationship between distraction index and the probability of development of osteoarthritis, with the steepest part of the curve often occurring when the distraction index is between 0.5 and 0.8.110 Despite the recognized association between laxity and the development of hip dysplasia, the relationship between the distraction index and the benefits of juvenile pubic symphysiodesis remains investigational. The dog is anesthetized, and the caudal abdomen and inguinal area are prepared for aseptic surgery. Juvenile pubic symphysiodesis is commonly combined with elective castration or ovariohysterectomy, so the exact margins for aseptic preparation depend on the combination of intended procedures. The dog is placed in dorsal recumbency, and a standard approach to the pubic symphysis is performed.97 In male dogs, the skin incision is made parallel to the penis and extends from just in front of the pubis caudally to the cranial edge of the scrotum. The subcutaneous fascia is incised, and collateral branches of the pudendal artery and vein are ligated; then the penis is retracted laterally to allow incision of the deep fascia and subperiosteal elevation of the origins of the adductor and gracilis muscles. In female dogs, the skin incision is made directly at the midline, and the subcutaneous fascia and adductor and gracilis muscles are separated in the same line. Cauterization of the pubic symphysis is performed with a standard cautery unit set at 40 W, with a unipolar electrode applied for 10 to 30 seconds at each cauterization point;91 this is repeated every 2 to 3 mm along the pubic symphysis (Figure 60-5). Only the cranial one third to one half of the symphysis should be ablated. Internal pelvic structures may be protected from excessive heat during cauterization by transrectal palpation by a gloved assistant, or by placement of a thin ribbon malleable retractor introduced into the pelvic canal from the cranial aspect of the pubis. Alternatively, the surgeon can make a small incision into the abdomen just cranial to the pubis and can monitor temperature by manual palpation from the cranial aspect of the pubis. Closure is performed in layers with reapposition of the adductor and gracilis muscles across the pubic symphysis used as the first layer, followed by closure of the subcutaneous fascia and then the skin. Rationale and Patient Selection Pelvic osteotomy, or triple pelvic osteotomy as it is commonly performed, is a prophylactic surgical intervention intended to decrease abnormal hip joint laxity, normalize articular stresses, and improve hip joint congruity (Figure 60-6) via joint remodeling. Rotation of the acetabulum provides greater acetabular coverage of the femoral head to ensure continuous hip joint reduction through a normal range of motion (Figure 60-7).113,114,124 Biomechanical studies suggest that triple pelvic osteotomy decreases the magnitude of the hip force and increases the contact area of the force application.24,25 Pelvic osteotomy was first described in the veterinary literature by Hohn and Janes in 1969.49 Many variations on the technique have been described over the past 50 years; however, the basic procedure described by Slocum is currently the most popular.123 Immature dogs clinically affected by hip dysplasia with palpable or radiographic joint laxity, but with no radiographic signs of secondary osteoarthritis, are candidates for triple pelvic osteotomy. Generally, dogs will be candidates up to approximately 10 months of age, when many dogs develop radiographic secondary osteoarthritis, but in rare cases, dogs do not develop secondary arthritis despite lax hip joints at maturity and thus remain candidates for the procedure. Some minimal coverage of the femoral head is a necessary criterion for surgery because dogs that have no acetabular capture of the femoral head at all continue to subluxate after triple pelvic osteotomy and are not candidates for correction (Figure 60-8). Triple pelvic osteotomy may be performed unilaterally or bilaterally, although the author recommends unilateral surgeries staged 4 to 6 weeks apart. Although controversial, the procedure is not recommended in dogs without clinical signs, as it is difficult to predict the exact degree of subluxation that will cause any dog to develop clinical hip dysplasia, or to what degree and at what age a dog will be affected. More reliable indices than direct palpation techniques should be used to predict clinical hip dysplasia if the procedure is to be performed in a dog without current clinical signs. The PennHIP distraction index provides a reliable assessment of hip joint laxity, and disease-susceptibility curves have been developed to provide information on the probability of developing radiographic evidence of hip osteoarthritis associated with a given distraction index. These curves provide the veterinarian and the owner with information regarding the probability that an individual will develop radiographic evidence of osteoarthritis based on laxity.110 However, the development of clinical osteoarthritis includes other factors, such as patient activity, breed, gender, weight, and age. Therefore, a variety of factors are included when one is considering whether triple pelvic osteotomy should be performed on dogs without clinical signs. Definitive recommendations for surgical intervention remain elusive according to the current literature. Hip joint laxity is best assessed clinically via an Ortolani test on a sedated or anesthetized dog (Figure 60-9).20 The animal is placed in dorsal recumbency with the stifle flexed and the femora held vertically. Pressure down the femoral shaft produces dorsal coxofemoral subluxation. While downward pressure is maintained, the femur to be examined is slowly abducted. In patients with subluxation, a click, known as the Ortolani sign, is produced during reduction of the femoral head into the acetabulum. Alternatively, the Ortolani test can be performed with the animal in lateral recumbency.20 One hand grasps the stifle and applies a proximally directed force to the femur, while the other hand stabilizes the pelvis. Abduction of the femur produces similar reduction of the femoral head. The angle of reduction roughly corresponds to the rotation of the acetabulum needed. Dogs with an angle of reduction smaller than 30 degrees are good candidates for triple pelvic osteotomy. Some surgeons recommend the use of 20 degree triple pelvic osteotomy plates exclusively, because an experimental study using a special hinged plate showed that stable reduction of dysplastic specimens consistently occurred for acetabular ventroversion angles of 20 degrees.25 Survey radiographs should be taken in Orthopedic Foundation for Animals (OFA) or PennHIP positions to confirm laxity and assess the degree of degenerative change. Triple pelvic osteotomy is an accepted, proven prophylactic treatment for hip dysplasia in immature dogs without secondary osteoarthritis. Clinical studies show consistent subjective improvement in dogs after triple pelvic osteotomy,81,82,113,114,124 with 92% to 93% satisfactory limb function noted postoperatively. Kinetic gait analysis is held by most surgeons, however, as the best objective measure for lameness outcomes.101 Kinetic gait analysis also has been used to confirm a high rate of positive outcomes after triple pelvic osteotomy surgery.56,82,128 Significant increases in peak vertical force of dysplastic limbs occur as early as 8 weeks after triple pelvic osteotomy, and values for peak vertical force reach normal by 28 weeks postoperatively. Although triple pelvic osteotomy provides a high rate of successful functional recovery, secondary osteoarthritis may progress after triple pelvic osteotomy, despite improvement in joint stability.56,60,81,128 Even when triple pelvic osteotomy does not consistently stop the progression of osteoarthritis, the resulting improvement in joint stability is usually sufficient to yield a functional outcome.103 A standard lateral approach to the ilium is performed.96 The origin of the deep gluteal muscle is elevated from the ilium. An ilial osteotomy is performed with an oscillating bone saw extending from just caudal to the caudal dorsal iliac crest perpendicular to the long axis of the ilium and perpendicular to the plane of the ilial surface (Figure 60-10). This perpendicular cut allows an exact rotation around the long axis. Alternatively, some surgeons make the osteotomy from just caudal to the caudodorsal iliac crest and directed caudoventrally toward the ventral margin of the ilium at a 30 degree angle to the long axis of the ilium. The caudal ilial segment is grasped with a bone-holding forceps such as a Kern bone-holding forceps, is rotated laterally, and is secured at the surgeon’s discretion for a side-specific pelvic osteotomy plate. As previously noted, 20 degree plates are sufficient for most patients.132 First, the plate is secured to the caudal ilial segment with cortical or cancellous screws, then cancellous screws are used in the cranial ilial segment, with the ventral screw placed in compression mode. Cranial screws that extend into the sacrum have traditionally been considered to be associated with a decreased possibility of screw loosening,121,137 but a recent report suggests that screw loosening occurs least when cancellous screws did not extend into the sacrum.29 Screw loosening was significantly less prevalent with self-tapping screws than with pre-tapped screws.77 Joint stability is assessed by testing the hip joint in a range of motion, including an Ortolani test. If instability persists, a plate with greater rotation can be substituted and a capsulorrhaphy performed, or a Lembert imbrication suture can be placed into the capsule to tighten the joint capsule. The pubic segment saved earlier is morselized and placed in the dorsal aspect of the osteotomy behind the rotated caudal ilium. The ischial hemicerclage wire, if placed, is now tightened to stabilize the ischial osteotomy. Both incisions are closed in standard fashion by surgeon preference. Figure 60-10 Location and orientation of pelvic osteotomies according to the procedure described by Slocum.122,123 The cranial ramus of the pubis is removed first (bottom inset), then an ischial osteotomy is performed (top inset); finally, a transverse ilial osteotomy is made immediately caudal to the caudal dorsal iliac crest (center) with the osteotomy oriented perpendicular to the long axis of the pelvis (dotted line). (From Schulz KS, Déjardin LM: Surgical treatment of canine hip dysplasia. In Slatter DH, editor: Textbook of small animal surgery, ed 3, Philadelphia, 2003, Saunders/Elsevier.) Some surgeons prefer to perform simultaneous bilateral triple pelvic osteotomys.13 For these procedures, the animal is placed in ventral recumbency, and both sides of the pubis are approached through a ventral midline incision; the pubic segments are removed bilaterally through the central incision. The animal then is placed in lateral recumbency and is surgically prepped, and a triple pelvic osteotomy is completed through caudal ischial and lateral ilial approaches, as previously described. Then the dog is flipped into the opposite lateral and surgically prepped, and the procedure is repeated. A technique variation for the triple pelvic osteotomy procedure has been described in which the stabilization provided by the pelvic osteotomy plate is supplemented with a dynamic compression plate placed on the ventral aspect of the ilial body.40 The purported advantages of this procedure include increased strength of fixation, less incidence of screw loosening, and less incidence of fixation failure. Disadvantages of the procedure include greater exposure and elevation of muscle from the ventral ilium, increased surgical time, and increased cost of the additional implants. In many commercial pelvic osteotomy plates, a wire hole is present in the caudal half of the plate that was initially intended to allow hemicerclage wire placement around the plate and the ilium to facilitate plate application. A retrospective study has shown that use of the wire has no effect on postoperative implant stability.121 Complications of triple pelvic osteotomy are primarily under the surgeon’s control. Poor surgical technique may result in damage to the sciatic or obturator nerve. Loosening of the cranial screws has been reported in up to 62% of dogs.60 Early weight bearing and weak juvenile bone are hypothesized as possible reasons for screw loosening.50,51 Screw loosening can be limited by the use of cancellous screws in the cranial segment, the use of longer screws that have purchase in the sacrum, and by strict exercise confinement after surgery.6 Ventral plate stabilization of the ilium and the pelvic osteotomy plate has been described and is highly effective in combating implant failure.40 Early detection of screw loosening has been advocated to allow prophylactic intervention and avoid complications.12 Obstipation and dysuria are reported complications secondary to narrowing of the pelvic canal.106 Obstipation and dysuria are avoided by removing the most lateral portion of the pubis and by using pre-angled side-specific commercial pelvic osteotomy plates rather than twisted conventional plates.45,69 Overrotation of the acetabulum has been reported to result in femoral neck impingement by the acetabular rim and decreased ability to abduct the hip.12,106,114,123 Selection of the minimal angle necessary to provide improved joint congruity is important to minimize complications of overrotation.24,25 Femoral head and neck ostectomy is a salvage surgical procedure for hip dysplasia that is intended to eliminate most of the pain caused by hip joint laxity in the immature dog, or pain due to secondary osteoarthritis in the mature dog. It is also used in the treatment of aseptic necrosis of the femoral head (Legg-Calvé-Perthes disease), fractures of the femoral neck or capital physis, coxofemoral luxation, and failed total hip replacement. Femoral head and neck ostectomy has also been referred to in previous literature as femoral head and neck excision, femoral head ostectomy, and femoral head excision, but femoral head and neck ostectomy is a more accurate term for what the surgery is intended to accomplish. Femoral head and neck ostectomy can be performed in dogs of any age but will likely result in better outcome if performed in toy- or small-breed (<20 kg) dogs than in large- or giant-breed dogs. Previous attempts to improve outcomes of femoral head and neck ostectomy by the interposition of various muscle flaps between the acetabulum and the remnant femoral neck have not proved beneficial, but clinical outcome will be enhanced by complete excision of the femoral neck67 and by immediate postoperative physical therapy to improve joint mobility and limb use. Dogs are candidates for femoral head and neck ostectomy if clinical signs of pain and lameness cannot be alleviated by analgesic therapy, weight loss, or other nonsurgical means, and if they are not candidates for, or economic or environmental conditions dictate against, other methods of surgical therapy such as triple pelvic osteotomy or total hip replacement. The functional outcome of femoral head and neck ostectomy may be affected by surgical technique, duration of clinical signs, patient age, postoperative care and physical therapy, body weight, and disease severity.32,44,75,92 Body weight is the most commonly investigated factor in outcome. Dogs weighing less than 17 kg have better results than larger dogs32,42,75,92; however, the surgery should be considered for larger dogs if total hip arthroplasty is not a surgical option, because femoral head and neck ostectomy still may result in improved quality of life if correctly performed. Patient age is not a consideration in otherwise healthy dogs; however, younger dogs generally have a better outcome than older dogs. Published reports of clinical results after femoral head and neck ostectomy have primarily consisted of the results of veterinarian observations or client questionnaires, but most show improvement in clinical signs for the majority of dogs. Objective gait analysis data have become available only recently for current research dogs.9,30,32,44 Functional changes after femoral head and neck ostectomy include decreased abduction and extension of the hip, limb shortening and dorsal displacement of the femur, decreased stifle and hock angulation, and muscle atrophy. Recovery from the procedure to maximal improvement in function may take 6 to 8 months, and the function of younger dogs improves faster than that of older dogs.9,92 Simultaneous bilateral femoral head and neck ostectomy has been reported and results in high levels of client satisfaction.104 The cause of the poorer outcome in larger dogs has not been determined. Some studies suggest that bone-on-bone contact from inadequate excision or postoperative formation of enthesophytes or ectopic bone is the primary cause of poor outcome68,129; others suggest that the bone contact is too common to explain differences in clinical outcome.31,33 Complete excision of the femoral neck, including removal of the lesser trochanter, may improve results.67 Numerous attempts have been made to interpose tissue between the acetabulum and the femoral neck to improve clinical outcome after femoral head and neck ostectomy, but results have been equivocal or negative.* Muscle transpositions using the biceps femoris,11,66,68 the deep gluteal muscles,9 and a vascularized rectus femoris muscle sling have been described. Ischiatic nerve damage has been reported in three dogs after biceps femoris or deep gluteal muscle flaps were used in combination with femoral head and neck ostectomy.55,100 Kinetic gait analysis has failed to demonstrate improvement in weight bearing when interpositions have been used.63,75 Muscle interpositions are no longer recommended clinically on a routine basis. If revision osteotomy is contemplated because of unacceptable bone-on-bone contact or extensive limb atrophy, muscle interposition may be used and outcome may be improved by the use of antibiotic prophylaxis, creation of a muscle flap base 1.5 times the width of the ostectomy surface, use of the caudal pass of the biceps femoris muscle flap, suturing of the muscle flap under minimal tension, suturing of the flap to the middle gluteal and vastus lateralis muscles, and careful identification and protection of the ischiatic nerve.64
Surgical Therapy of Canine Hip Dysplasia
Anatomy
Selection of Appropriate Surgical Options
Juvenile Pubic Symphysiodesis
Rationale, Patient Selection, and Timing
Surgical Approach and Procedure
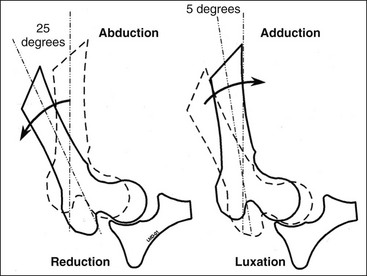
Pelvic Osteotomy
Evidence
Surgical Approach and Procedure
Technique Variations
Complications of Triple Pelvic Osteotomy
Femoral Head and Neck Ostectomy
Rationale, Patient Selection, and Timing
Evidence
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


