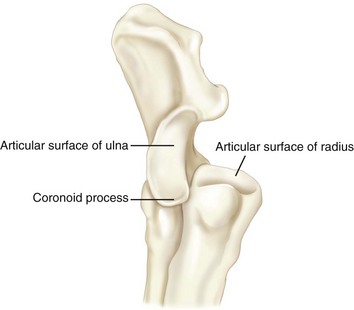
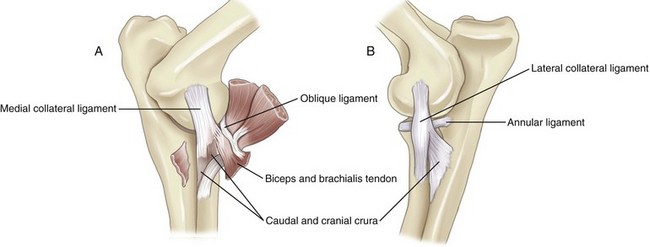
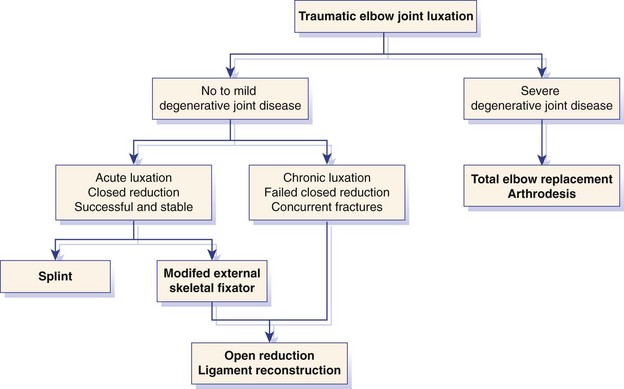
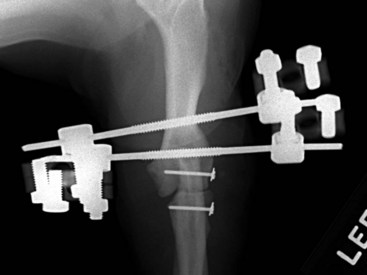
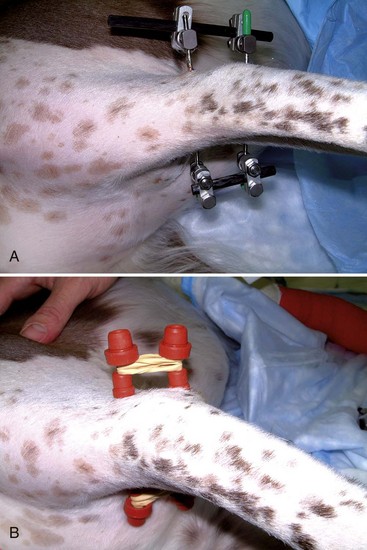
Chapter 53 The elbow joint comprises three synovial joints: humeroradial, humeroulnar, and proximal radioulnar joints. The humeroradial joint transmits most of the weight-bearing forces of the limb, the humeroulnar joint restricts the movement of the joint to a sagittal plane, and the radioulnar joint allows for rotational (pronation and supination) movement.13,38 The radius is the main weight-bearing bone of the forearm (antebrachium) with articular surfaces at both the proximal and distal ends.38 However, the proximal articular surface of the ulna was found to contribute substantially to the transfer of loads through the canine elbow joint, supporting 48% to 49% of forces applied on normal cadaveric forelimbs.90 The articular circumference of the radius is longer than the corresponding trochlear notch to allow for rotation of the elbow joint.38 Although the proximal radius initially was believed to provide most of the weight-bearing surface of the combined radial and ulnar joint surfaces, it later was found to carry about 51% to 52% of the forces applied to the elbow joint.90 Therefore, the proximal articular surface of the ulna appears to contribute substantially to load transfer through the canine elbow joint. The ulna articulates with the humerus, at the level of the trochlear notch, the anconeal process, and the medial portion of the coronoid process.38 The medial and lateral portions of the ulnar coronoid process increase the surface area of the elbow joint and restrict the degree of freedom of its range of motion to the sagittal plane.38 The humeral capitulum articulates with the radial head, and the humeral trochlea articulates with the ulna, primarily the medial portion of the coronoid process. 6,38 The trochlea sits slightly distal and is larger than the capitulum. The larger size of the trochlea becomes important in discussion of the pathogenesis of the fragmented medial portion of the coronoid process. The trochlear notch of the ulna ends distally with the radial incisure. The lateral aspect of the medial portion of the coronoid process contacts the radial head along its incisure (Figure 53-1). The base of the medial portion of the coronoid process articulates with the radial head and the humeral trochlea, extends into an intermediate section or midbody, and ends in an apex located distal to the radial head (see Figure 53-1). The medial portion of the coronoid process diverges distally in a caudal to cranial direction and medially at the level of the apex. The normal range of motion of the elbow joint is approximately 130 degrees, with normal limits being approximately 36 degrees (range, 34 to 38 degrees) in flexion and 165 degrees (range, 164 to 167 degrees) in extension, as measured via goniometry in awake Labrador Retrievers.71 The range of motion of the elbow is limited in torsion and in the mediolateral plane by the anconeal process and by the presence of collateral ligaments (Figure 53-2). When the elbow joint is extended at 135 degrees, the anconeal process articulates with the olecranon fossa to act as the only primary stabilizer in pronation. In this position, the lateral collateral ligament provides primary stabilization for supination, the anconeal process, and the medial collateral ligament, playing secondary and tertiary roles, respectively.152 When the elbow and the carpus are held at 90 degrees, the medial collateral ligaments are responsible for the rotational stability of the elbow joint. Their integrity is therefore tested in that position with the use of Campbell’s test.18 Although this test has been validated in cadavers, the rotational range of motion of the elbow joint varies greatly between individuals, in both dogs and cats.40 When these ligaments are intact, the paw can be rotated anywhere from 17 to 50 degrees laterally (supination) and from 31 to 70 degrees medially (pronation), depending on the source.18,40,117 The proximal attachment of the medial collateral ligament is at the medial epicondyle of the humerus and divides into the cranial and caudal crura, respectively, while attaching distally to the radius and the ulna. The medial collateral is weaker than the lateral collateral ligament. The lateral collateral ligament has a proximal attachment at the lateral epicondyle of the humerus and splits in a similar fashion as the medial ligament.138 The annular ligament prevents cranial translation of the radius in relationship to the ulna due to attachments on the proximal radius, and the ulna. The annular ligament lies deep to the collateral ligaments.38 The interosseous ligament extends across the interosseous space between the radius and the ulna. All of these ligaments lie external to the joint capsule, which encompasses the joint and forms cranial and caudal compartments. The joint capsule is composed of an inner synovial layer and an outer fibrous membrane. Conflicting information has been obtained regarding the presence of a fibrous joint capsule at the caudal aspect of the elbow joint in the dog, with the authors of one study indicating that no fibrous joint capsule is present in this region.23,38 Extension of the elbow joint is achieved by contraction of muscles attaching to the olecranon and consisting essentially of the triceps brachii muscle. The anconeus and the tensor fasciae antebrachii muscles act as tensors of the antebrachial fascia and contribute to the action of the triceps brachii muscle. These extensor muscles are innervated by the radial nerve. Flexion of the elbow joint relies on muscles localized to the anterior aspect of the limb, consisting mainly of the biceps brachii and brachialis muscles. The tendon of insertion of the biceps brachii muscle splits into a stronger band attaching to the ulnar tuberosity, and a weaker band inserting to the radial tuberosity.38 The terminal tendon of the brachialis muscle inserts between these two bands as a large flat tendon of insertion on the ulnar tuberosity. Recently, these muscles have been proposed to contribute to the pathogenesis of medial coronoid disease by creating shear forces along the radial incisure.41 The extensor carpi radialis muscle arises at the lateral epicondylar crest of the humerus and extends to the distal limb. This muscle appears to contribute to flexion of the elbow joint during the swing phase of the gait.157 Flexion of the elbow joint is dependent upon innervation provided by the musculocutaneous nerve. The regional anatomy of the elbow has been presented in a pictorial review.23 When approaching the elbow medially, care should be taken to avoid the median nerve and the associated branch of the median artery, both of which lie beneath the pronator teres muscle at the craniomedial aspect of the joint. In the cat, these structures run through the humeral supracondylar foramen.118 The ulnar nerve and the collateral ulnar artery should be identified when an osteotomy of the olecranon is performed. These structures can often be palpated superficially, as they cross the caudomedial aspect of the joint before they continue distally between the flexor carpi radialis and superficial digital flexor muscles. The radial nerve courses craniolateral to the joint, with the deep branch running under the proximocranial border of the extensor carpi radialis muscle.38 Traumatic luxation of the elbow joint is uncommon in dogs and rare in cats because of the inherent stability provided by the bony conformation and strong muscular and ligamentous structures surrounding this joint.7,108,135 The anconeal process interlocks in the olecranon fossa, preventing luxation unless the elbow joint is flexed beyond 45 degrees. The distal slope and the relatively large size of the trochlea of the humerus prevent medial displacement of the radius and ulna, explaining why 90% of elbow joint luxations are oriented laterally.18 Fracture of the distal humerus or proximal radius and ulna is more common; when associated with a radial head luxation, it is referred to as a Monteggia fracture. Elbow joint luxations are believed to result from rotational forces transmitted to the joint via musculotendinous structures.108 Although collateral ligament damage has been reported in 18% to 50% of clinical cases, a recent in vitro study found that elbow joint luxation in dogs was not possible unless at least the lateral collateral ligament was transected.18,40,108,135 In cats, luxation of the elbow joint required transection of both medial and lateral collateral ligaments. Elbow joint luxations therefore should be expected to be associated with soft tissue disruption of the joint capsule, rupture or avulsion of one or both collateral ligaments, and articular cartilage damage. In cases of severe injury, the origins of the flexor or extensor muscles also may be ruptured or avulsed from the humeral condyle. A diagnosis of elbow joint luxation is confirmed on a craniocaudal radiographic projection and is based on lateral (or medial) translation of the radius and ulna (Figure 53-3). With complete luxation, the antebrachium may be displaced proximally owing to contracture of the triceps brachii muscle. In approximately 16% of cases, the anconeal process remains in the olecranon fossa, with the olecranon caudolateral and the radial head lateral to the joint.135 Radiographs are closely evaluated for the presence of avulsion fractures or articular fractures that may preclude closed reduction as a means of treatment. Secondary osteoarthritis may be present with chronic luxation or in patients with preexisting disease. As soon as preoperative assessments are complete and no contraindications are identified, the patient can be anesthetized safely and treated according to the algorithm proposed in Figure 53-4. Closed reduction is especially relevant for treatment of acute luxation of a joint that appears to be otherwise normal. The prognosis is not as favorable in dogs with chronic luxation, failed closed reduction, or preexisting disease. Closed reduction is contraindicated in cases of concurrent intra-articular or periarticular fracture. Salvage procedures may be considered for elbow joints with severe degenerative joint disease. After reduction, the joint is assessed both radiographically and physically for instability (Figure 53-5). Radiographic evidence of mild radial head subluxation is interpreted carefully. Mild signs of laxity could be attributed to muscle relaxation under anesthesia, as documented in human beings.74 Stress radiographs with the limb extended and placed in varus and valgus may help to fully document the degree of elbow joint instability. Collateral ligament integrity can be determined by manipulating the extended elbow joint in a varus or valgus direction, or by flexing the carpus and elbow joint to 90 degrees and rotating the antebrachium, as was first proposed by Campbell in 1969 and validated by Farrell in 2007.18,40 Campbell’s test is performed with the elbow joint and carpus at 90 degrees of flexion to position the anconeal process caudal to the olecranon fossa, so that rotational stability of the elbow joint relies primarily on the collateral ligaments. The anconeal process has been found to act as the primary rotational stabilizer in pronation if the elbow joint is extended to a standing angle of 135 degrees.152 In flexion, pronation of normal cadaver canine elbow joints approached a mean of 30 degrees (range, 17 to 40 degrees), and supination averages 46 degrees (range, 31 to 67 degrees).40 Transection of the medial collateral ligament increases pronation to 60 to 100 degrees, whereas transection of the lateral collateral ligament increases supination to 70 to 140 degrees.18,40 Angles of pronation and supination appear to vary widely between individuals, with the range of motion correlating inversely with the weight of the animal.40 The degree of laxity of the reduced elbow joint should therefore be compared with that of the normal contralateral elbow joint when the integrity of the collateral ligaments is assessed. The incidence of collateral ligament injury associated with elbow joint luxation varies between studies. Some authors report collateral ligament injury in 18% to 50% of luxations.18,108,135 It is interesting to note that normal elbow joints could not be luxated unless at least the lateral collateral ligament was transected in a cadaver experiment.40 However, traumatic elbow joint luxation may be associated with elongation rather than disruption of the collateral ligaments. This would explain why a successful outcome can be obtained even when mild to moderate instability is present after closed reduction of the elbow joint. In normal feline cadaver elbow joints, the mean angle of pronation increased from about 50 degrees (30 to 70 degrees) to 99 degrees after transection of the medial collateral ligament. Supination increased from nearly 130 degrees (108 to 150 degrees) to 167 degrees after sectioning of the lateral collateral ligament.40 In this experiment, luxation of feline elbow joints was not possible unless both collateral ligaments were transected. If marked physical or radiographic evidence of varus or valgus instability is found, an open approach with reconstruction of the collateral ligament is indicated. Otherwise, conservative management and immobilization of the joint in extension can be attempted. Open reduction is indicated in cases of avulsion fracture of the humerus at the site of collateral ligament attachment, articular fracture, intra-articular interposition of soft tissues, marked instability or reluxation after closed reduction, and chronic luxation (Figure 53-6). Chronic luxations are often associated with marked fibrosis and contracture that prevent closed reduction. Although elbow joint luxation is rare in cats, open reduction and reconstruction of soft tissues is usually indicated. This recommendation is based on experimental evidence indicating that elbow joint luxation in this species requires transection of both collateral ligaments, as well as on a case report and the author’s personal clinical impressions.7,40 The goals of open reduction are to reduce the luxation, to assess articular surfaces, and to reconstruct the collateral support structures. Salvage procedures may be considered as an alternative treatment for severely degenerative elbow joints or chronic luxation. The elbow joint is treated via a caudolateral approach.117 The skin incision extends from the distal third of the humerus to the proximal third of the ulna, cranial to the olecranon. The lateral epicondyle of the humerus usually is difficult to palpate as a landmark because of the lateral displacement of the ulna and radius. If the anconeus muscle has not been lacerated in the injury, a myotomy may be used to further approach and enter the joint. Hemorrhage is minimized if the muscle can be elevated from the olecranon by subperiosteal dissection. The articular surfaces are inspected and the antebrachium manipulated to lever the anconeal process over the lateral epicondylar crest to engage the olecranon fossa. Muscle relaxation and placement of a clamp to allow caudal traction on the olecranon facilitate reduction. A blunt or Freer periosteal elevator can be used to lever the radius and ulna medially, with caution taken to avoid damage to the articular surface. The use of a fracture distractor anchored in the distal humerus and proximal ulna has been proposed to displace the ulna distally in difficult cases.32 After reduction, the joint is thoroughly lavaged and elbow joint stability assessed using Campbell’s test, as was previously described for closed reduction. Reconstruction of supporting soft tissues (joint capsule, muscles, and collateral ligament) is indicated if there is any doubt as to the stability of the joint. Collateral ligaments can be reconstructed by primary repair with augmentation or ligament replacement with synthetic materials.7,18,108 The lateral collateral ligament can be approached through a caudolateral incision, but access to the medial collateral ligament requires a separate medial approach to the elbow joint. Midsubstance tears tend to be sutured primarily with nonabsorbable suture material in a locking loop or similar pattern, with or without augmentation with synthetic materials or autogenous tissue.18 Avulsions of humeral attachments of the collateral ligaments can be reattached through transverse bone tunnels in the humeral epicondyle. Alternatively, they may be anchored using screws and spiked washers. Avulsions of the distal attachment of the collateral ligaments are sutured to the annular ligament and surrounding fibrous tissues. Avulsion fractures at the proximal or distal ligament attachment may allow placement of a small lag screw or a tension band device if the fragment is of sufficient size.32 Damaged ligaments tend to be friable and offer poor holding properties for suture repair. Therefore, ligament replacement is often indicated as an adjunct to primary repair of collateral ligaments, or as a sole repair technique, if the ligaments cannot be sutured. Prosthetic replacement of collateral ligaments requires placement of screws and washers, or bone anchors, at the sites of attachment in the humeral epicondyle and radial neck (Figure 53-7). Heavy nonabsorbable suture is looped over each screw in a figure of eight pattern. Nylon, polypropylene, or a braided polyblend suture (FiberWire, Arthrex Inc., Naples, FL) may be used. Following repair, stability is reassessed and surrounding soft tissues inspected. The flexor or extensor muscle groups are occasionally avulsed from their origin on the humeral epicondyle. If this occurs, they are reattached to the surrounding periosteum and fibrous tissues prior to routine closure of the fascia and subcutaneous and cutaneous tissues. Cases with medial and lateral collateral ligament rupture may be managed by a technique that relies on transcondylar tunnels and biaxial suture repair.40 A humeral transcondylar bone tunnel is drilled, starting at the humeral attachment of the lateral collateral ligament, immediately craniodistal to the lateral epicondyle of the humerus, and directed to a point immediately craniodistal to the medial epicondyle. A guide wire may be used to ensure adequate placement before the tunnel is drilled with a cannulated drill bit. A transradial tunnel is created in a lateral-to-medial direction at the attachment of the lateral collateral ligament on the radial head. A transulnar tunnel is created at the level of the midportion of the ulnar trochlear notch, midway between the articular surface and the caudal ulnar cortex. A double loop of braided polyblend suture (FiberWire) is threaded through the humeral tunnel and cut so that one end is passed through each of the distal tunnels. Sutures are tied with half-hitch knots, with the elbow joint maintained in a standing position. Postoperative management depends on the severity of the injury, the method of repair, and the client’s compliance. External coaptation is indicated after closed reduction to maintain the limb in extension, thereby relying on locking of the olecranon into the olecranon fossa to prevent recurrence. Adjunct fixation is also indicated following open reduction and repair of collateral ligament(s) to allow fibrosis and healing of supporting structures. This recommendation is supported by a nondestructive biomechanical study in which cadaver elbow joints were approached medially with transection of the medial collateral ligament. Operated elbow joints retained only 19% of their original stiffness, and all medial collateral ligament repairs failed from suture pull-out.141 These findings support the need for adjunct fixation after repair of torn collateral ligaments. Although transarticular pinning has been described,108,124 the standard of care currently consists of providing external support in the form of a splint or a modified external skeletal fixator. In patients with acute luxation and mild residual instability, the application of a well-padded bandage or splint (spica) for 2 to 3 weeks is recommended.108,135,139 After removal of the bandage or splint, clients are encouraged to initiate rehabilitation measures. Strict exercise restriction is enforced for the first 4 to 6 weeks, but nonforceful passive range of motion exercises and controlled limb use are promoted. The benefits of early mobility of the joint include decreased adhesions between periarticular structures, stimulation of the synthesis of glycosaminoglycans and hyaluronate, encouragement of more orderly collagen deposition and normal cross-linkage, improved joint nutrition, and improved clearance of the joint hematoma.32,89 Prolonged immobilization (≥3 weeks) decreases synovial fluid production, as well as cartilage stiffness and thickness, and leads to degenerative joint disease and loss of muscle mass and bone mineral content.14,105 To avoid these limitations, flexible external skeletal fixation has been proposed to maintain the reduction of elbow joints with mediolateral instability.139 This technique requires placement of two centrally threaded pins of appropriate diameter parallel to the articular surface of the elbow joint. One full pin is placed in the distal humerus, proximal to the supratrochlear foramen, and the other is placed through the center of the olecranon (Figure 53-8; see also Figure 53-7). The elbow joint is held at approximately 140 degrees of extension while the two pins are fixed to connective bars on the medial and lateral aspects of the joint. Rubber plugs (such as blood sampling tube stoppers) are driven over the pins before and after placement of the elastic bands to prevent migration of the bands, friction against the skin, and other injuries. This rigid frame is maintained until postoperative swelling has decreased, or longer in cases of chronic elbow joint luxation. The connective bars can then be replaced by tight elastic bands on the medial and lateral aspects of the elbow to allow range of motion (see Figure 53-8). A soft-padded bandage should be applied to the limb and changed once daily until soft tissue swelling has resolved. The pin tracts should be cleaned daily initially and as needed after removal of the bandage, and the frame should be checked twice daily after the elastic bands have been placed. Owners should be instructed to watch for migration of the bands or signs of wear and tear. At this point, physical therapy should include warm compresses, passive range of motion exercises, and cold packing. Only short leash walks are allowed, followed by massage of the limb. The flexible external skeletal fixator is usually removed within 3 to 4 weeks after surgery. The outcome following treatment of elbow joint luxation has not been assessed objectively, most likely because this condition is uncommon. The prognosis is typically considered as good to excellent when the luxation is treated early, stability is achieved after closed reduction, and physical rehabilitation is started early. One retrospective study reported good to excellent results in about 89% of 35 dogs treated with closed reduction.108 In another study, a good to excellent outcome was attained in only 8 of 19 dogs (47%) with closed reduction, largely because of residual instability in 7 of these 19 joints.135 Therefore, the prognosis is affected by the severity of cartilage and soft tissue damage, duration before repair, degree of persistent instability, and compliance of the client. The most common major complication after a closed reduction is reluxation, warranting open reduction and repair of the collateral ligaments. The most common complication likely consists of degenerative joint disease, observed in all cases in a small retrospective study with long-term follow-up.7 Owners therefore should be informed of the likelihood of decreased range of motion and advised about preventive measures against osteoarthritis.7 The most common complication specific to flexible fixation of the elbow joint is excessive drainage and infection around the pin tracts.139 This complication seems more likely to occur when flexible fixation is applied within 2 to 3 days after surgery, before postoperative swelling has resolved. Other complications include fracture of the olecranon (Figure 53-9), premature pin loosening, pin breakage, and deterioration of the bands. Congenital luxation of the elbow joint is an uncommon anomaly, accounting for about 15% of all nontraumatic elbow lameness in the dog.116 A radiologic classification proposed in 1982 divided congenital elbow joint luxations into three types.78 Type I is characterized by a lateral or caudolateral dislocation of the radial head with the ulna in a relatively normal location (Figure 53-10). This condition is more common in young, medium- to large-breed puppies and results in mild deformity and loss of function. The congenital origin of this type of luxation has been questioned because of its similarity to luxations secondary to trauma or asynchronous growth between the radius and ulna.97 Type II is the most common type of chronic elbow joint luxation and involves disruption of the humeroulnar articulation with lateral rotation and subluxation or luxation of the ulna, occasionally associated with a dislocation of the radial head (Figure 53-11). This condition affects primarily small-breed dogs and is associated with limb deformity and severe disability at a very young age. Type III consists of luxation of the radius and ulna. This condition has no known breed predisposition but is frequently associated with generalized joint laxity (polyarthrodysplasia) and multiple congenital skeletal deformities, such as ectrodactyly. Therefore, treatment is rarely initiated. Caudolateral luxation of the radial head seems more common in large-breed dogs. Isolated cases or case series have reported the problem in the Afghan Hound, Golden Retriever, Bull Mastiff, Collie, Boxer, Old English Sheepdog, Bulldog, Doberman Pinscher, and Shetland Sheepdog.78,98,151 Although less common, this type of luxation has been described in Yorkshire Terriers, and the author has diagnosed it in a Dachshund.150 Affected puppies may show slight external rotation (supination) of the antebrachium, a valgus deformity at the carpus, and mild lameness. Because of their mild nature, these signs usually are not noticed by owners until puppies reach 3 to 4 months of age. The radial head can be palpated lateral to the joint on physical examination, and the range of motion of the elbow joint is limited. Muscle atrophy, pain, and crepitus often develop with time. A definitive diagnosis of caudolateral luxation or subluxation of the radial head is established with radiographs of the elbow (see Figure 53-11). Other findings may include a convex articular fovea of the radial head, hypoplasia of the proximal radial diaphysis and epiphysis, lateral angular deformity of the proximal radial diaphysis, angular deformity of the distal humerus with a trochlea extending farther distal than normal, medial deviation and distortion of the olecranon, and cranial curvature of the proximal ulna.78,98,150,151 Secondary osteoarthritis is present in chronic cases. Conservative treatment is an option in dogs with mild clinical signs. Patients should be closely monitored until maturity (see Figure 53-11). Monthly orthopedic examinations are indicated to monitor limb conformation and lameness; serial radiographs are obtained to evaluate joint congruence and continued growth, particularly at the distal ulnar physis. Delaying treatment until skeletal maturity may be advantageous to limit the risk of limb-length discrepancies caused by damage to growth plates. However, delaying surgery increases the risk of irreversible changes such as remodeling of the articular surfaces and degenerative joint disease. Therefore, surgical treatment is recommended based on severity of pain, progressive subluxation of the elbow joint, and remodeling of the radial head.147 Surgical options include open reduction and stabilization, radial head ostectomy, and arthrodesis. Open reduction is performed through a lateral approach to the proximal radius.118 An oblique osteotomy or ostectomy distal to the radial physis may be indicated to facilitate reduction. Care is taken to avoid detachment of the proximal radial epiphysis during reduction in younger patients. The joint is stabilized by reconstruction of the lateral collateral ligament and joint capsule in younger patients with mild disease. More severe conditions may necessitate another means of fixation, such as application of bone plates or an external skeletal fixator (see section on traumatic elbow joint luxation) or placement of a screw or pin between the proximal radius and ulna. Surgical synostosis between the ulna and the radius is contraindicated in young and rapidly growing dogs, as this will lead to joint incongruity and potential limb angulation. Resolution of muscle atrophy and normal function were reported in a 4-month-old Dalmatian puppy with type I chronic elbow joint luxation treated with a modified Bell-Tawse procedure.150 This surgical intervention included four steps: (1) dissection of the soft tissues surrounding the radial head and humeral condyle through a lateral approach radial, (2) wedge ostectomy and counterclockwise rotation of the proximal radius, followed by plate fixation to align load transmission along the axis of the radius, (3) reconstruction of the annular ligament with a muscular fascial strip obtained from the extensor carpi ulnaris muscle (modified Bell-Tawse procedure), and (4) temporary (20 days) humeroradial fixation with a transarticular Kirschner wire. Although further evaluation of this technique is indicated, the approach may be superior to radial head ostectomy, which usually results in poor outcome.32 Arthrodesis of the elbow joint generally is successful in relieving pain but induces a marked gait abnormality. It is considered a superior alternative to amputation and is reserved for chronic dislocations and joints with severe degeneration. Joint replacement has not been reported as a treatment option. Congenital elbow joint luxation is currently considered a contraindication to joint replacement (Loic Dejardin, personal communication). Radiographs obtained immediately following surgery are evaluated to assess joint alignment and implant positioning. Depending on the method of fixation, a well-padded bandage or spica splint may be applied for 7 to 10 days. If weight bearing is not desired, a carpal flexion bandage may be used to allow passive range of motion of the elbow joint and rehabilitation. Transarticular pins and external skeletal fixators are usually removed after 2 to 3 weeks. If an external skeletal fixator (see section on traumatic luxations) is used, frequent evaluations of the pins and apparatus are necessary to correct possible complications quickly. Physical therapy is encouraged as soon as possible after the elbow joint is stable. Judicious use of swimming, stair climbing, and frequent nonforceful passive manipulation helps restore flexion and extension. Exercise should be limited to leash walks for 4 to 6 weeks. Lateral rotation/luxation of the ulna affects predominantly small purebred dogs such as Yorkshire Terrier, Boston Terrier, Shetland Sheepdog, Miniature Poodle, Pekingese, Miniature Pinscher, Pomeranian, Pug, Cocker Spaniel, English Bulldog, and Chihuahua.8,17,97,98 The thoracic limb deformity is typically noted at birth or shortly thereafter, along with variable degrees of lameness. Partial joint flexion and internal rotation of the antebrachium characterize the posture. Bilaterally affected dogs may almost cross their thoracic limbs and be forced to bear weight on the caudal or caudomedial aspects of the elbows and antebrachium. The olecranon can be palpated lateral to the distal humerus, limiting extension of the joint with little to no pain response. Radiographic findings include craniolateral rotation of the proximal ulna with a relatively normal humeroradial articulation and a narrowed radial neck (see Figure 53-10). The anconeal process and the medial portion of the coronoid process are variably present, and more severe manifestations include lateral displacement of the radial head. In chronic cases, other changes include muscle atrophy and remodeling of the humeral epicondyles, trochlear notch, and olecranon fossa.78 Following reduction, recurrence is prevented by placement of a transarticular pin or a modified external skeletal fixator.97,139 Transarticular pinning requires placement of one or two small threaded Kirschner wires from caudal to cranial through the semi-lunar notch into the distal humerus. Pins are cut flush with the skin but with enough pin protruding to permit removal 14 to 21 days later.174 The modified external skeletal fixator technique is described in the section on traumatic elbow joint luxation. This approach is indicated in dogs over 4 to 5 months of age, or when closed reduction fails. The caudolateral approach to the elbow joint provides adequate exposure, and osteotomy of the olecranon is rarely indicated.118 Maintenance of reduction can be accomplished by a variety of means, including medial imbrication, transposition of the olecranon medially and distally, ulnar osteotomy and radioulnar synostosis, trochlea and trochlear notch reconstruction, external fixation, and transarticular pins.17,97,98,139 If the trochlea and trochlear notch are fairly congruent, lateral release, medial imbrication, and distomedial olecranon transposition/modified external fixation may be sufficient to maintain reduction. Elbow dysplasia is a syndrome that includes several conditions that result in incongruence of the joint, eventually leading to degenerative joint disease. In 1993, the International Elbow Working Group (IEWG) agreed that “elbow arthrosis caused by fragmented coronoid process (FCP), osteochondrosis (OC[D]), ununited anconeal process (UAP), articular cartilage anomaly, and/or joint incongruity is the manifestation of inherited canine elbow dysplasia.” Elbow dysplasia is a common inherited condition affecting 17% of Labrador Retrievers94,102,103 and up to 70% of Bernese Mountain Dogs in the Netherlands.62 This disease is bilateral in 35% of affected dogs. Without treatment, elbow dysplasia will inevitably lead to the development of osteoarthritis in the affected joint, producing lameness in juvenile, mainly large- and giant-breed, dogs. The high prevalence and the devastating effects of degenerative joint disease of the elbow justify the need for preventive screening and early treatment. Breeds predisposed to ununited anconeal process consist of large to giant dogs, such as the Bernese Mountain Dog, German Shepherd Dog, Golden Retriever, Labrador Retriever, Mastiff, Newfoundland, Rottweiler, and Saint Bernard Dog.84 In a study of breed susceptibility to developmental orthopedic diseases based on data retrieved from 10 hospitals, odds ratios for ununited anconeal process were greatest in Bernese Mountain Dogs and Mastiffs.84 Other breeds affected by ununited anconeal process include Great Danes, French Bulldogs, Dachshunds, and Weimaraners.144 Ununited anconeal process is bilateral in 20% to 35% of affected dogs, and male dogs are affected twice as frequently as female dogs.61,144 Most dogs present with lameness between 5 and 12 months of age; however, with bilateral disease, owners may not initially identify affected dogs. A subpopulation of mature animals with ununited anconeal process was reported as an incidental finding. Fragmentation of the medial portion of the coronoid process has been reported in 13% of elbow joints with ununited anconeal process, based on arthrotomy or arthroscopy.94 Seventy-two percent of dogs in this study were German Shepherd Dogs, with an overall male-to-female ratio of 2 : 1. Seventy-seven German Shepherd Dogs were diagnosed with ununited anconeal process. Additionally, radioulnar incongruence was diagnosed in 50% of cases, with a radioulnar step greater than 5 mm in five elbow joints.94 The anconeal process articulates with the humerus by engaging the supratrochlear foramen from the olecranon fossa. This process provides stability to the elbow joint by limiting mediolateral movement when engaging the humerus. The anconeal process in small-breed dogs does not have a separate center of ossification.29 In large-breed dogs, especially German Shepherd Dogs, Mastiffs, Basset Hounds, Bloodhounds, and Greyhounds, the anconeal process develops as a single separate center or as several small centers of ossification within the process.144 In a longitudinal study examining the radiographic appearance of canine elbows, this fusion normally occurred at 14 to 15 weeks in Greyhounds. Fusion occurred later in German Shepherd Dogs, at between 16 and 20 weeks of age.55 In this study, postmortem evaluation of dogs with ununited anconeal process documented the presence of an easily movable anconeal process surrounded by osteophytes. Osteophytosis appeared more frequent and more pronounced on the ulna than on the radius or humerus. Compared with other conditions associated with elbow dysplasia, the ununited anconeal process led to formation of the greatest number of osteophytes, and the severity of changes correlated with the age of the dog. The pathogenesis behind lack of fusion of the anconeal process remains unclear. Nutritional deficiencies, genetic disturbance of growth-stimulating hormones, growth rate, and trauma to the physis have all been advocated as potential causes.158 In a study of elbow dysplasia in German Shepherd Dogs, three dominant genes were proposed in the transmission of these traits in that breed.29 Ununited anconeal process has also been described as a manifestation of osteochondritis dissecans, with a disturbance in endochondral ossification leading to epiphyseal lysis and ununited anconeal process.30,144 The microcirculation may become disrupted during ossification, leading to subsequent separation in the weakened cartilage, thus preventing bony union.111 The most recent literature describes elbow joint incongruity, radioulnar (short radius syndrome) incongruence, or an abnormally shaped trochlear notch as a likely cause of ununited anconeal process.144,158,171,172 Damage to the distal ulnar physis is the most common cause of asynchronous growth of the radius and ulna. In this instance, the ulna becomes shorter than the radius, thereby decreasing the distance between the anconeal process and the radial head compared with normal joints.143 If the radial head is located proximal to the medial portion of the coronoid process, the humeral condyle shifts proximally, leading to excessive force on the developing anconeal process. Repeated microtrauma would damage the center of ossification, leading to failure of union.143 This hypothesis is supported by clinical reports of fusion of the anconeal process in young dogs with ununited anconeal process treated by proximal ulnar osteotomy.143 A second theory proposing elbow joint incongruity as a cause of ununited anconeal process proposes that a reduction in shortening of the vertical distance between the anconeal process and the radial incisure (decreasing the radius of the trochlear notch) leads to poor articulation between the ulna and the humeral condyle. The disparity between the size of the trochlear notch and that of the humeral condyle was found to increase the loading of the anconeal process, thus preventing its bony union.143 Wind hypothesized in 1986 that if the proximal ulna does not grow faster than the humeral condyle, elbow joint incongruence secondary to an elliptically shaped notch can occur.171 A diagnosis of ununited anconeal process is made easily based on physical examination findings and radiographic changes (Figure 53-12). Dogs with ununited anconeal process present with gradual onset of weight-bearing unilateral or bilateral forelimb lameness that is generally chronic and worse after exercise. Joint effusion tends to be more profuse than with medial compartment disease and can be detected by palpating over the caudolateral aspect of the joint. Pain is elicited during palpation of this region and during extension of the joint. Radiographic views should include mediolateral, craniocaudal, and hyperflexed lateral projections. The maximally flexed lateral radiograph helps diminish the superimposition of the humeral epicondyles over the anconeal process and the distal humeral physis.27,158 An area of lucency is apparent between the anconeal process and the proximal ulna in elbows in which a ununited anconeal process is present. Other radiographic changes may include periarticular osteophyte production, joint distention, muscle atrophy, and irregular subchondral sclerosis.138 Osteophyte production tends to be faster and more pronounced with ununited anconeal process than with fragmentation of the medial portion of the coronoid process or osteochondritis dissecans, and most osteophytes are located in the proximal region of the ulna.55 Radiographs of both elbows should be obtained because of the incidence of bilateral disease. Radiographic diagnosis should not be made until after the dog is 22 to 24 weeks of age. Advanced imaging or arthroscopy is recommended to assess the presence of concurrent lesions in the medial compartment of elbow joints with ununited anconeal process. It should also be noted that use of the lateral radiographic projection, which is ideal for identifying ununited anconeal process, causes superimposition of the coronoid processes.94 Advanced imaging such as computed tomography or arthroscopy may be considered for diagnosis of concurrent elements of elbow dysplasia. The traditional surgical treatment for ununited anconeal process consists of excising the affected process through a caudolateral approach, with a midbelly incision through the anconeus muscle. The fragment is grasped with pointed bone forceps or a towel clamp, and surrounding soft tissue attachments are excised. Early intervention is recommended to optimize functional outcome and minimize the postoperative progression of degenerative joint disease. A retrospective study of dogs with ununited anconeal process treated by surgical excision reported that 90% of owners were satisfied with their dogs’ level of activity after surgery and rated the outcome as good to excellent.130 Another study of 16 dogs with a mean follow-up of 19.5 months after surgery reported a normal degree of elbow joint flexion in 58% and normal extension in 84% of operated dogs.144 Although owners appeared satisfied with the surgical outcome, only 50% of dogs were free of lameness. The postoperative prognosis seems to vary with the measures of outcome tested, and owners should be warned of the progression of degenerative joint disease (50% of dogs were free of lameness).144 An objective evaluation of function following excision is warranted. Use of force plate analysis to quantitatively measure function in the operated limb compared with unoperated or disease-free limbs would provide a better measure of outcome. Surgical reattachment of the anconeal process has been proposed as an alternative treatment for ununited anconeal process in dogs younger than 24 weeks of age with a normally formed ulnar notch.158 The procedure is performed via a lateral approach to the elbow, and the fragment bed is debrided prior to implant placement. The anconeal process is fixed to the proximal ulna by placement of lag screws or Kirschner wires. The implants can be driven from the articular surface or from the caudal aspect of the ulna into the anconeal process. Exact positioning is important, as deviation from the normal position can induce contact between the anconeal process and the olecranon fossa, thus increasing the risk of implant failure.144,158 Union between the anconeal process and the proximal ulna was obtained 2 to 6 months after surgery in six of ten dogs evaluated retrospectively.47 These results are encouraging, but the value of the study is limited by its small sample size. Another therapeutic strategy for ununited anconeal process addresses elbow joint incongruity as the underlying cause of ununited anconeal process and involves an ulnar osteotomy performed alone or in combination with reattachment of the anconeal process (Figure 53-13). The rationale behind this procedure relies on contraction of the triceps brachii muscle to pull the ulna proximally during weight bearing. This proximal migration of the ulna is expected to restore the natural alignment of joint surfaces, thereby alleviating the biomechanical loads applied on the anconeal process. Restoration of congruity by ulnar osteotomy can encourage union between the anconeal process and the ulna.143 The osteotomy is traditionally located 30 to 60 mm distal to the radial head joint surface and is created through a limited caudal approach to the ulna. This proximal location has been recommended to facilitate the proximal migration of the ulna but may be associated with higher morbidity.119,158 Indeed, a distal osteotomy did not restore the radioulnar contact patterns in an experimental model of incongruity, presumably because the interosseous ligament prevents migration of the proximal ulna relative to the radius.119 The postoperative tendencies for caudal tipping of the proximal ulna and varus deformation can be minimized by orienting the osteotomy in an oblique plane: The osteotomy starts at a proximal, caudal, and lateral point and aims for a distal, cranial, and medial position, about 40 to 50 degrees to the long axis. Alternatively, an intramedullary pin may be placed in the medullary canal of the ulna to maintain the axis of the ulnar displacement.106 The most common complication associated with this approach is pin migration. In a study of 21 dogs treated with ulnar osteotomy, the anconeal process healed to the ulna in 15 cases, but a radiolucent line persisted in 6 cases.143 Seventeen dogs had a good to excellent clinical outcome. Only one dog had severe osteophytosis on radiographs, and most osteophytes were present before surgery. Results were less favorable in another study of 17 dogs, in which lameness was improved in 21 of 23 elbows, but only 5 of 23 anconeal processes achieved postoperative union.159 Ulnar osteotomy has been combined with internal fixation of the anconeal process, but additional studies are warranted to evaluate the benefits of this procedure. Only one study reported on long-term outcome in 4 dogs, all with excellent clinical results.83 Ununited medial humeral epicondyle was first described in 1966 and was later defined as failure of the medial epicondyle ossification center to unite with the distal humerus.88,151 The distal portion of the humerus develops from three centers of ossification, which are responsible for growth of the trochlea, capitulum, and medial epicondyle, respectively. The medial epicondyle normally fuses with the humerus by 6 months of age and forms the point of origin of flexor muscles of the carpus and digits. Others attributed this disease to an osseous metaplasia of the flexor tendons, traumatic avulsion of the flexor tendons, osteochondritis dissecans of the humeral trochlea, or development of an aberrant center of ossification.54,95,117,177 Ununited medial humeral epicondyle is generally considered an uncommon condition in dogs, although a prevalence of 15% was recently reported in a cohort study of 7 litters (48 dogs) of Labrador Retrievers.115 The authors suggested that this disease may be underdiagnosed because pets are not routinely screened for elbow disease, and this lesion is not readily apparent on the mediolateral radiographs currently required for elbow screening by the Orthopedic Foundation for Animals (OFA). However, all reports agree that young Labrador Retriever s seem most predisposed, followed by German Shepherd Dogs and English Setters.35,95,117 When present, clinical signs associated with ununited medial humeral epicondyle are similar to those seen with osteochondrosis/osteochondritis dissecans of the elbow joint. The diagnosis is based on radiographic evidence of a discrete osseous structure on the medial aspect of the elbow joint. Single or multiple mineralized fragments varying in number and size are detected on craniocaudal views of affected elbow joints (Figure 53-14). A few reports describe growth of the bony fragments over time in adult dogs, including recurrence after surgical excision.117,169,177 The condition may be accompanied by adjacent bone defects. Ununited medial epicondyle can occur concurrently with elbow dysplasia but remains considered as a separate entity, because it can present as the only abnormality diagnosed in affected elbows.115 Figure 53-14 Radiograph of an elbow with ununited medial epicondyle. A large osseous fragment is present medial to the joint.
Surgical Diseases of the Elbow
Anatomy
Traumatic Luxation of the elbow joint
Diagnosis
Treatment
Closed Reduction and Stabilization
Open Reduction and Stabilization
Joint Immobilization and Aftercare
Prognosis and Complications
Congenital Luxation of the elbow joint
Caudolateral Luxation of the Radial Head
Treatment
Aftercare
Lateral Rotation of the Ulna
Closed Reduction and Immobilization
Open Reduction and Immobilization
Elbow Dysplasia
Ununited Anconeal Process
Pathogenesis and Pathophysiology
Diagnosis
Treatment and Outcome
Ununited Medial Humeral Epicondyle

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Surgical Diseases of the Elbow








Only gold members can continue reading. Log In or Register to continue
