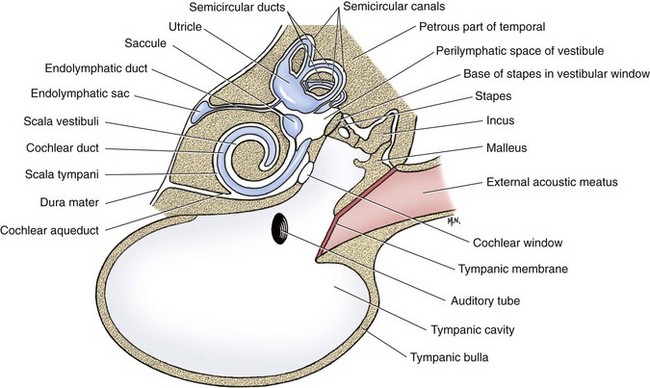
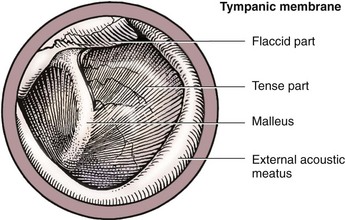
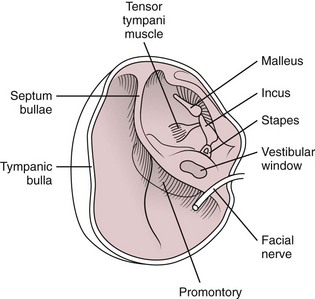
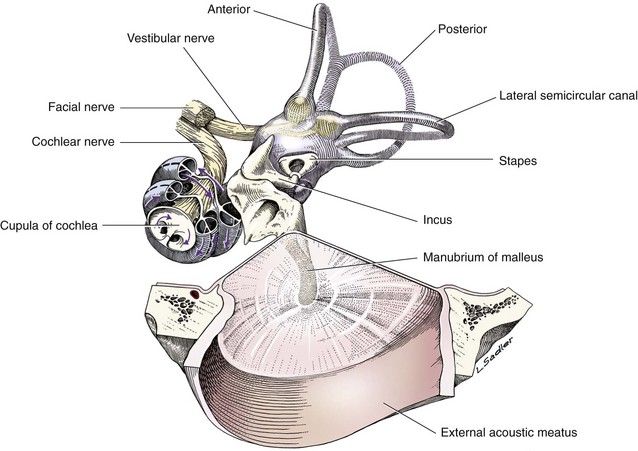
Chapter 123 The tympanic cavity, formed by the tympanic component of the temporal bone, is a bony shell situated caudal and medial to the zygoma and temporomandibular articulation. The cavity has dorsal, middle, and ventral compartments (Figure 123-1) and is lined with respiratory mucosa contiguous, via the auditory tube, with that of the nasopharynx. The combined volume of the compartments is related to body weight.21 The dorsal component—the epitympanum or epitympanic recess—is the smallest of the three chambers and is largely occupied by the incus and part of the malleus. It is lined with cuboidal or squamous epithelium with few cilia. The middle component—the mesotympanum or true tympanic chamber—is a four-sided chamber lined with columnar or cuboidal epithelium and variable numbers of ciliated cells. The middle chamber is bounded laterally by the larger of two tympanic membranes, which separates it from the external ear; the smaller secondary membrane (the cochlear membrane) is located posteriorly within this chamber. On the medial aspect of the middle chamber, level with the tympanic membrane, is found the bony promontory that accommodates the cochlear structure. The ventral component of the tympanic cavity, termed the hypotympanum, is the largest of the chambers and is situated within the tympanic bulla, the spherical bone prominent ventrally. It communicates with the tympanic cavity proper through an anterolateral-facing elliptical opening on its dorsal aspect and is lined with cuboidal or squamous cells. Despite variations in the thickness of the bulla wall, which is thickest on its rostral and lateral aspects, the chamber’s interior profile remains regular. Two membranes are found within the mesotympanic chamber: the tympanic membrane and the secondary cochlear (or round) membrane. The tympanic and cochlear membranes separate the chamber from the external acoustic meatus laterally and the inner ear medially, respectively. The tympanic membrane is a thin, translucent, triple-layered structure with contributions from the external and middle ear. The membrane is divided into the smaller pars flaccida and larger ventral, pars tensa (Figure 123-2). The pars flaccida occupies the dorsal portion of the membrane and covers a small area of the middle ear chamber that, in dogs, is separated from the remainder of the epi- and mesotympanum. The pars tensa comprises the majority of the membrane; the manubrium of the malleus is embedded in its dorsal aspect. The membrane is constructed of an inner epithelium derived from the pharyngeal pouch, a central fibrous layer also of pharyngeal origin, and an outer stratified squamous epithelium derived from the ectoderm of the outer ear. Its longitudinal axis slopes so that its ventral aspect is more medial, and its outer surface is concave because of its attachment to the malleus. The outer epithelial cells originate at the attachment of the malleus and migrate peripherally from this point to the external auditory meatus; this continual centrifugal movement of cells clears debris from the surface of the membrane and is also responsible for its repair in the event of rupture. The opening to the auditory tube, also known as the eustachian or pharyngotympanic tube, is found in the rostral mesotympanic chamber. The tube is a short structure connecting the tympanic chamber with the nasopharynx. Its length varies from 1 to 2 cm, and its oval lumen between 1 and 2 mm in diameter. The wall of the tube is supported medially in the nasopharyngeal region by cartilage, in the tympanic region by the petrous temporal bone, and laterally by the tensor veli palatini muscle. The tube is lined with ciliated, pseudostratified, or columnar mucosa. Its middle segment has mainly ciliated cells that progress to a combination of goblet cells, nonciliated columnar cells, and ciliated cells at the tympanic opening. Mucus and goblet cells predominate at the pharyngeal end. Cannulation of the auditory tube via the pharyngeal opening for drainage purposes is feasible.41 The feline middle ear has a similar overall anatomic arrangement to that of dogs; however, its chambers show much more distinct separation into a larger ventral cavity (Figure 123-3), the hypotympanum, and a smaller rostrolateral component corresponding to the epitympanum and mesotympanum. The two components are almost completely separated by a bony septum and communicate on their medial aspect through a small slitlike opening that widens into a distinct foramen caudally. This separation gives rise to the characteristic “double shell” profile of the tympanic structures visible on anteroposterior radiographic views. The lining of the chambers is reported to contain more abundant ciliated and secretory cells than in dogs. The distribution of neural structures within the middle ear is similar to that in dogs. On entering the middle ear, the tympanic plexus distributes widely across the bony promontory but is reported to be more exposed, or possibly more sensitive, to iatrogenic trauma. The bony labyrinth is a perilymph-filled cavity in the temporal bone that communicates with the middle ear via the vestibular and cochlear windows. It contains the membranous labyrinth, which is divided into three sections (Figure 123-4): the vestibule, cochlea, and semicircular canals. The vestibule is the middle portion of the labyrinth and contains the saccule and utricle of the membranous labyrinth. The cochlea is a bony, spiral “seashell” structure containing the cochlear coil. The coil originates at the cochlear window and is divided by the cochlear duct, which forms a shelf across the cochlea, into two sections: the scala vestibuli and the scala tympani. The floor of the duct is formed by the basilar membrane, which contains the organ of Corti. There are three interconnecting, fluid-filled semicircular canals: anterior, lateral, and posterior. Each has an ampulla arranged at right angles to the others. The saccule and utricle are found at the confluence of the canals. The precise mechanism by which bacteria are able to gain access to the tympanic chamber is still unresolved. Although it has always been assumed that the tympanic membrane must be damaged to permit ingress of microorganisms, various authors have shown that the membrane is intact or even thickened in many dogs with septic otitis media.49,52 This finding may support the possibility of transmembrane migration by the bacteria; it is equally conceivable, however, that temporary perforation and subsequent repair of the membrane permits ingress. Alternatively, bacterial invasion of the integument that lines the osseous external auditory prominence and surrounds the membrane may explain their ingress to the middle ear. This is supported by the fact that the predominance of canine breeds affected by septic otitis media reflects that of dogs prone to otitis externa. In patients with chronic otitis externa, however, microbial flora of the external meatus and their antimicrobial susceptibility differ considerably from those organisms responsible for septic otitis media.9,40 The most commonly encountered microorganisms in canine middle ear infections are reportedly Staphylococcus intermedius, Pseudomonas spp., and Malassezia yeast.9 Cryptococcal infection of the tympanic chamber has been reported in cats.4 Other conditions that permit bacterial access to the middle ear include foreign body perforation and traumatic disruption of the external acoustic meatus. Not only may foreign bodies damage the tympanic membrane, but persistence of the foreign body in the external meatus and tympanic chamber can prevent its normal repair. Traumatic disruption at the level of the annular cartilage may be encountered as the result of bite wounds in dogs and cats. The subsequent inflammatory process may seal off the horizontal component of the external meatus adjacent to the tympanic membrane from the remainder of the meatus, effectively trapping bacteria within a secretory environment. The resultant abscessation disrupts the membrane, which allows the infection to spread to the middle ear and gives rise to para-aural discharge.59 Para-aural abscessation can also occasionally occur as a sequela to iatrogenic stenosis of the external meatus after lateral wall resection or from residual integumentary remnants left within the bulla after total canal ablation.67 Rarely, congenital atresia of the external acoustic meatus may lead to a similar disease process within the bulla. Pathologic changes recognized in the middle ear as a consequence of established bacterial infection include thickening of the tympanic membrane, and epithelial hyperplasia with thinning of the lamina propria and the development of associated granulation tissue.49 A lymphoid and polymorphonuclear leukocyte infiltrate is usually evident. The wider availability of sectional imaging has allowed an increasing recognition of the incidence of extension of septic otitis media to involve the inner ear and adjacent intracranial structures.60,72 Inflammatory polyps are non-neoplastic masses that originate from the epithelium of the tympanic chamber or auditory tube. The condition is most frequently recognized in, and is the most important middle ear disease, of cats but it is also occasionally recognized in dogs.64 Polyps may remain within the bony confines of the middle ear chamber, extend into the nasopharynx (Figure 123-5), or disrupt the tympanic membrane and appear in the external acoustic meatus (Figure 123-6). The condition is encountered more frequently in young cats and is often preceded by an episode of upper respiratory viral infection. Experimental ligation of the auditory tube in cats has also been shown to result in polyp development; thus, it seems likely that an inflammatory episode, resulting in obstruction of drainage, is a possible underlying cause of the abnormal epithelial reaction.73 Figure 123-5 Middle ear inflammatory polyp in the cat: nasopharyngeal mass. The palate is being retracted dorsally. Cholesteatomas are characterized by destructive and expanding keratinizing squamous epithelium. In dogs with septic otitis media, epithelium may undergo metaplastic changes, producing connective tissue and even new bone proliferation in more advanced cases.49 There may be glandlike areas within the granulation tissue that, because of their cystic structure and the presence of cholesterol clefts, have been likened to the condition recognized in humans as cholesteatoma. A congenital form has not been reported in dogs; most appear to be acquired after an episode of otitis media.19,20,32,39,51 Inadvertent instillation of some antiseptic and ceruminolytic agents through a disrupted tympanic membrane has been shown to give rise to a sterile inflammation of the tympanic chamber and, in some cases, hearing loss and vestibular damage.42–44,56 Congenital anomalies of the middle ear are uncommon; agenesis of the whole or part of the tympanic membrane is occasionally recognized. Congenital anomalies of the inner ear resulting in hearing or vestibular dysfunctions have been reported in a number of breeds,70 including collapse of the scala media in the Dalmatian,7 neuroepithelial degeneration in Rottweilers,16 and changes in the organ of Corti in Pointers.15 Secretory (Serous) Otitis Media Secretory otitis media is characterized by accumulation of mucinous material within the tympanic chamber and is an increasingly recognized syndrome, particularly in Cavalier King Charles spaniels.18,66,69 This condition, often referred to as “glue ear” in children, results in impaired conductive hearing function. Dysfunction of the auditory tube itself may lead to increased negative pressure, allowing accumulation of mucous secretion within the tympanic cavity. An underlying cause has not been identified. Although upper respiratory viral infections are implicated in humans, the breed-related incidence in dogs suggests a congenital dysfunction of drainage via the auditory tube. Dogs that present with congenital hypoplasia or malformations of the soft palate are reported to be at risk for middle ear disease and impaired hearing function.36,77 Primary ciliary dyskinesia, a rare congenital condition resulting in depressed ciliary function, has been reported in dogs.28 In normal animals, active mucociliary function of the tympanic lining removes debris trapped in mucus via the auditory tube. Loss of this function leads to failure of middle ear drainage. One of the many consequences, therefore, of this generalized ciliary dysfunction is sterile otitis media. The majority of tumors involving the middle ear are usually identified as extensions of neoplasms derived from structures of the external ear canal; tumors derived from structures of the tympanic cavity and auditory tube are rare. Tumors of true tympanic origin include ceruminous gland adenocarcinomas,48,53 squamous cell carcinoma,31,79 carcinoma of unknown origin, and lymphoma.22 Neurologic signs (i.e., Horner syndrome, vestibular signs) indicating extension to involvement of the middle ear are occasionally recognized in dogs with malignancy of the external ear but are more commonly encountered in cats. Tumors of the inner ear are extremely rare, and many patients presented with vestibular signs are ultimately found to have central lesions. Most patients with otitis media do not exhibit neurologic signs; however, tympanic inflammation may affect any of the nerves within the tympanic chamber. Possible neurologic changes therefore include facial nerve palsy and Horner syndrome. The incidence of facial palsy in dogs with established otitis media is reported to be approximately 10%.49 It is characterized by impaired palpebral function and facial and aural drooping. The extratympanic component of the facial nerve may also be affected if otitis media is severe enough or by the inflammatory changes caused by chronic otitis externa. The incidence of Horner syndrome is somewhat lower than that of facial involvement and is an unusual sign of middle ear disease; signs include ptosis, miosis, enophthalmos, and protrusion of the nictitating membrane. Damage to parasympathetic fibers carried in the chorda tympani may also lead to reduced tear secretion and promote keratitis sicca. However, it is unclear if disease processes involving the other functions of the chorda tympani and tympanic nerve, including salivary innervation, would always be clinically apparent. Otitis media may progress to involve the inner ear. Otitis interna may result in hearing loss and vestibular signs; further extension to affect the intracranial structures may give rise to symptoms of central vestibular disease, altered mentation, abnormal posture, cranial nerve deficits, and seizures.60,68,72
Middle and Inner Ear
Anatomy of the Middle Ear
Cats
Anatomy of the Inner Ear
Pathophysiology of Middle and Inner Ear Disease
Inflammatory Diseases of the Middle Ear

Cholesteatomas
Congenital Anomalies
Disorders of Middle Ear Drainage
Ciliary Dyskinesia
Neoplastic Disease
Presentation
Neurologic Signs
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Middle and Inner Ear

Only gold members can continue reading. Log In or Register to continue
