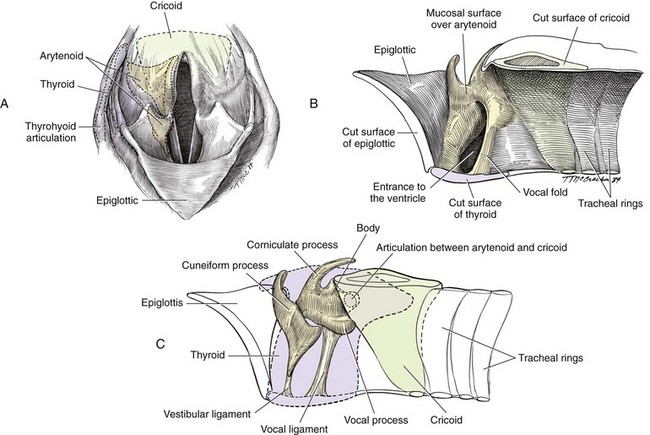
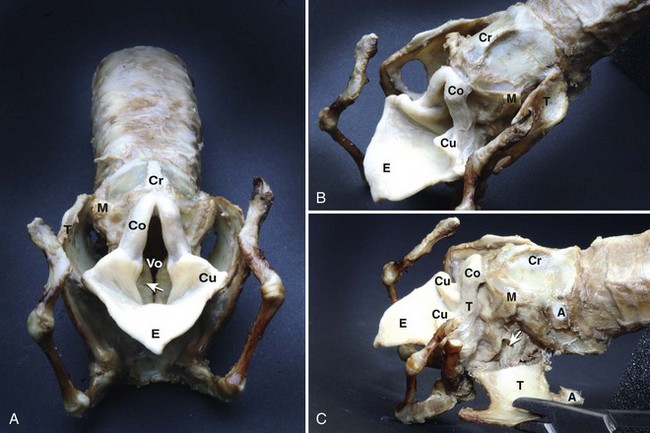
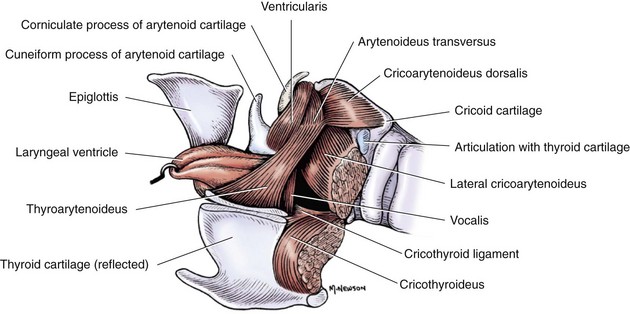
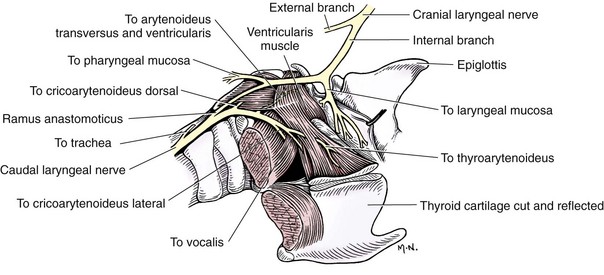
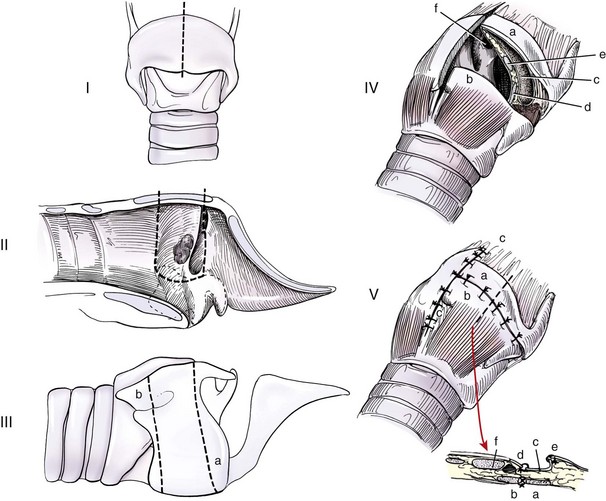
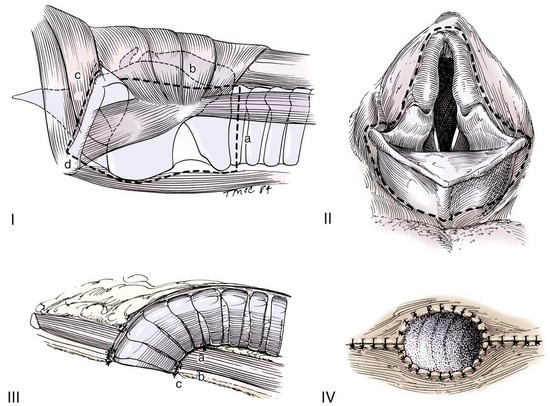
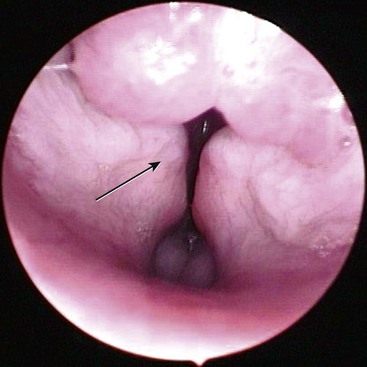
Chapter 101 The larynx is attached to the first ring of the trachea and is suspended ventral to the esophagus by the hyoid apparatus (Figures 101-1 and 101-2). Structurally, it is formed by epiglottic, thyroid, cricoid, sesamoid, interarytenoid, and paired arytenoid cartilages.28 The epiglottis is the rostral most cartilage. It is spade shaped, with its apex pointing rostrally and resting on the soft palate when in normal position. The oral (rostroventral) surface of the epiglottis is attached by a short, stout hyoepiglotticus muscle to the middle of the body of the hyoid bone.2,3 A thick stalk of fibrous tissue also unites the midcaudal portion of the epiglottis and dorsal rostral surface of the thyroid cartilage. Laterally, it attaches to the cuneiform processes by aryepiglottic mucosal folds. The thyroid cartilage is the largest laryngeal cartilage.27 It consists of right and left laminae that cover the sides of the larynx and fuse ventrally to form a short deep trough. Dorsally, the laminae expand to form thin rostral and caudal processes called cornua (Latin for “horns”), which are separated from the thyroid lamina by notches. The cranial laryngeal nerve and laryngeal artery pass through the rostral thyroid notch. Along its caudal border, the thyroid cartilage is united with the cricoid cartilage by the cricothyroid ligament. The cricoid cartilage forms a complete ring that is connected caudally to the first tracheal ring. The dorsal part of the cricoid cartilage is wide and thick with a median crest for muscle attachment. The cricoid cartilage has faceted articulations with the thyroid cartilage caudally and the arytenoid cartilage rostrally. Articulation sites are enclosed in articular capsules, forming synovial joints.27 The paired arytenoid cartilages consist of cuneiform, corniculate, vocal, and muscular processes.27 The triangular-shaped cuneiform process is the most rostral. Its ventral aspect lies in the aryepiglottic fold, and its dorsal aspect forms the midportion of the laryngeal inlet. The ventricular ligament and ventricularis muscle attach to the cuneiform process. The corniculate process forms the dorsal margin of the laryngeal inlet. It is horn shaped and lies caudal to the cuneiform process. The corniculate processes may be connected dorsally to each other by a sesamoid cartilage. Lateral to the cricoarytenoid articulation is the muscular process, which serves as the insertion site for the cricoarytenoideus dorsalis. The caudal ventral portion of the arytenoid cartilage contains the vocal process, which serves as an attachment of the vocal ligament and, from the thyroid cartilage, the vocalis muscle. Mucosal-covered folds over the ventricularis and vocalis muscles are separated by a region of everted mucosa known as a ventricle or laryngeal saccule.27 The larynx has extrinsic and intrinsic musculature (Figure 101-3).27 Extrinsic muscles include the thyropharyngeus and cricopharyngeus. The thyropharyngeus muscle is a large, flat muscle that covers the outside of the larynx; it extends from the lateral surface of the thyroid cartilage and inserts on the median raphe of the dorsal pharynx. It is innervated by glossopharyngeal and vagal nerves and functions to constrict the caudal part of the pharynx. The cricopharyngeus muscle has the same innervation and function as the thyropharyngeus muscle. It lies on the larynx and pharynx immediately caudal to the thyropharyngeus muscle, arising from the lateral surface of the cricoid cartilage and inserting on the median dorsal raphe of the pharynx. Along the caudal margin, some of the cricopharyngeus muscle fibers blend with the esophagus. The intrinsic muscles are responsible for laryngeal function.27 The most important muscle is the cricoarytenoideus dorsalis, which is responsible for abducting the arytenoid cartilage to open the glottis. This muscle arises from the dorsolateral surface of the cricoid cartilage and inserts on the muscular process of the arytenoid. The cricoarytenoideus lateralis muscle originates from the craniolateral surface of the cricoid cartilage and inserts on the muscular process of the arytenoid cartilage. It functions to pivot the arytenoid cartilage inward to close the rima glottis. The thyroarytenoideus muscle gives rise to ventricularis and vocalis muscles. It arises from the internal midline of the thyroid cartilage and inserts on the arytenoid cartilage, primarily on the deep surface of the muscular process. The vocalis portion of this muscle draws the arytenoid cartilage downward, relaxing the vocal cords, and the ventricularis portion constricts the glottis and dilates the laryngeal saccule. The arytenoideus transversus originates on the muscular process of the arytenoid and travels dorsally to insert at the interarytenoid cartilage. Some of its fibers blend with the dorsal aspect of the ventricularis muscle, enabling it to assist with vocal fold adduction and glottis constriction. The small, spindle-shaped hyoepiglotticus muscles extend from the ceratohyoid bone and fuse to form a single band that attaches on the ventral midline of the epiglottis. Contraction of these muscles draws the epiglottis downward.2,3 The cricothyroideus muscle is a thick muscle that lies laterally between the thyroid lamina and cricoid cartilage. When contracted, it pivots the cricoid cartilage on its thyroid articulation, tensing the vocal cords. Innervation to the larynx is provided by cranial and caudal laryngeal nerves (Figure 101-4), which originate from the vagus nerve.27 The cranial laryngeal nerve leaves the vagus at the distal ganglion and passes ventral to the larynx. It provides an external branch that supplies the cricothyroideus muscle and an internal branch that receives sensory fibers from laryngeal mucosa cranial to the vocal folds and serves as the afferent limb of the cough reflex. The internal branch of the cranial laryngeal nerve usually anastomoses with the caudal laryngeal nerve. The caudal laryngeal nerve is the terminal segment of the recurrent laryngeal nerve. The left recurrent laryngeal nerve from the left vagus arches around the aorta, ascends along the trachea, and gives off the pararecurrent laryngeal nerve before terminating as the left caudal laryngeal nerve. The right recurrent laryngeal nerve from the right vagus loops around the right subclavian artery and ascends along the trachea to end as the right caudal laryngeal nerve. The caudal laryngeal nerves provide motor supply to all intrinsic laryngeal muscles except for the cricothyroideus. Blood supply to the larynx is primarily through branches of the cranial and the caudal thyroid arteries. Lymphatic drainage is through the medial retropharyngeal lymph nodes.27 Unlike in dogs, feline arytenoid cartilages lack cuneiform and corniculate processes.23 True aryepiglottic folds are absent; instead, mucosa connects the sides of the epiglottis directly to the cricoid lamina. Whereas the vestibular folds are thin and sharply edged, the vocal folds are thick and rounded. Ventricles are absent, but pouches of the vestibule extend lateral to the vestibular folds. The larynx has three functions. During swallowing, the larynx and hyoid apparatus are pulled cranially, bringing the rima glottis under the epiglottis to block the laryngeal opening. The larynx is also responsible for controlling airway resistance, primarily by decreasing airway resistance with abduction of arytenoid cartilages during inspiration. Finally, the larynx is responsible for voice production by changing tension on vocal cords. In cats, rapid narrowing and widening of the glottis by laryngeal muscles and fast twitching of the diaphragm cause vibrations of respiratory air that result in purring.23 Laryngeal neoplasia is rare in dogs and cats, with most information in the literature from individual case studies. Reported tumor types in dogs include rhabdomyoma (oncocytoma), osteosarcoma, chondrosarcoma, melanoma, undifferentiated carcinoma, fibrosarcoma, mast cell, adenocarcinoma, and squamous cell carcinoma.* In cats, lymphoma and squamous cell carcinoma are the most common tumor types, although adenocarcinoma and poorly differentiated round cell tumor have also been reported.98,100,111,125 No breed or sex predilection has been documented in small animals. In dogs, ages at presentation range from 2 to 12 years of age, with oncocytoma appearing in younger adults.86,100 Cats are usually older, with ages ranging from 7 to 16 years.111 Most laryngeal tumors are locally invasive with a potential to metastasize. Oncocytomas do not readily metastasize; however, they are very locally aggressive.86 Presenting signs of animals with laryngeal tumors include respiratory stridor, exercise intolerance, dysphagia, gagging, coughing, progressive voice change, and dyspnea that does not improve with open-mouth breathing.100,110,111,125 Acute upper airway obstruction can occur with inflammation, edema, and accumulation of airway secretions within the trachea. In these patients, a temporary tracheostomy may be required to provide an airway while further diagnostics are performed. The diagnosis of laryngeal tumors is confirmed with laryngeal examination and mass biopsy. An upper airway mass may be visible on radiographic or ultrasonographic (echolaryngography) evaluation of the head and neck region. Thoracic radiographs are recommended for the detection of metastasis and aspiration pneumonia. The treatment depends on the mass size and tumor type. Lymphoma is controlled with radiation therapy or chemotherapy. Survival times in one study of three cats treated with chemotherapy were 60, 180, and 1440 days.111 In another study, eight of nine cats with laryngeal lymphoma responded to chemotherapy, with complete remission noted in seven cats.110 In that study, the survival time ranged from 16 to 330 days (median, 173 days). Small benign masses, along with their mucosal attachments, can be resected via a transoral approach or through a ventral laryngotomy (see “Debarking”).125 Larger or more aggressive tumors can be treated with partial or a complete laryngectomy.10,49,51 Partial or segmental laryngectomy is performed for tumors invading one side of the larynx and one vocal cord. The larynx is exposed through a ventral midline incision, and the thyroid cartilage is incised on the midline to gain access to the lumen. After determining the tumor limits, a segmental resection is performed. Tumors limited to the vocal cords are excised by standard vocal cordectomy (see “Debarking”) with primary closure of the mucosal defect. Tumors extending beyond the vocal cords are resected with removal of the vocal cord and a full-thickness portion of thyroid cartilage (Figure 101-5).81 Small cartilage defects can be primarily closed by sliding the cranial part of the thyroid cartilage caudally. Incision of the thyroid cartilage is continued from the resection site to the dorsal cartilage margin. The cranial segment of the thyroid cartilage is moved caudally and sutured to the caudal segment. The laryngeal mucosa is trimmed to prevent overlap as the thyroid cartilage is sutured. If resection requires removal of cricoid cartilage, the defect can be reconstructed by advancing the trachea cranially under the cricoid cartilage to the thyroid cartilage. The tracheal and laryngeal mucosa are aligned, and the cricoid and tracheal cartilage are held together with interrupted sutures. The cricothyroid muscles are sutured to the trachea to provide an air-tight seal, improve blood supply, and strengthen the anastomosis.81 Large cartilage defects can be repaired with use of free tissue implants (costal cartilage, buccal mucosa) or local muscle flaps. A “rotary door” procedure has also been used to bring vascularized epidermis into the laryngeal defect with the support of a myocutaneous flap.25,26,75 An island skin flap based on the sternohyoideus muscle is elevated, taking care to leave the skin attached to underlying muscle. During exposure of the trachea and larynx, the cranial thyroid blood vessels must be spared because they provide blood supply to the flap. After the laryngeal and tracheal resection is completed, the skin island is reduced to an appropriate size to fit the defect, and its epidermis is shaved off to remove hair follicles. The flap is rotated so that the dermis is facing inward and the dermis, subcutaneous tissues, and muscle edge are sutured to the resection site with the dermis flush with the mucosal lining. Suture knots are placed external to the airway. The dermal surface becomes covered with squamous or respiratory epithelium, with hair regrowth prevented by adequate epidermal shaving.25,26 For large tumors that involve both sides of the larynx, a complete laryngectomy with a permanent tracheostomy is required to palliate the clinical signs. There are few reports of complete laryngectomy in dogs and cats; thus, the success rate of this surgery is unknown.10,20,51 The skin is incised on midline, and the thyropharyngeus, cricopharyngeus, sternothyroideus, and thyrohyoideus muscles are detached from the larynx (Figure 101-6).81 The sternohyoideus muscle is left intact. Four stay sutures are placed in the fourth tracheal ring. The trachea is detached from the cricoid cartilage, and a sterile endotracheal tube is inserted in the distal trachea. The larynx is then dissected from the surrounding tissue without damaging the esophageal wall or innervation to the esophagus or pharynx. Dissection is carried from caudal to cranial. The larynx is detached from the hyoid apparatus, and the oral mucosa is incised around the rima glottidis. The pharyngeal mucosa is closed with an inverting pattern of 3-0 monofilament absorbable suture. Transected ends of the paired thyropharyngeus and cricopharyngeus muscles are sutured together ventral to the esophagus and pharynx without compressing the esophagus. The trachea is brought through the sternohyoideus muscles and to the skin. The tracheal wall is trimmed so the new orifice is oval in shape and rests flush with the skin. A round piece of skin can be removed to provide an opening larger than the trachea so the final closure will not result in tissue folds. The stay sutures are removed, and the trachea is anastomosed to the skin with a simple continuous suture pattern. Drains are placed if dead space or hemorrhage is present, and the subcutaneous tissues and skin are closed routinely. A gastrostomy tube is recommended for postoperative feeding until the site is healed. See Chapter 102 for management of tracheostomy sites. Brachycephalic breeds are those with short, wide heads. Rostral shortening of the skull may be accompanied by other defects that increase upper airway resistance, resulting in a condition termed “brachycephalic syndrome.” Brachycephalic syndrome encompasses a number of primary defects, most commonly stenotic nares (43% to 85%) and elongated soft palate (86% to 96%).68,90,91,94,113 Other primary defects include redundant pharyngeal folds, hypoplastic trachea, and nasopharyngeal turbinates.34,90,94,113 With turbulent airflow and increased negative inspiratory pressure secondary to narrowed airways, secondary changes such as everted laryngeal saccules (55% to 59%) and laryngeal collapse (8% to 70%) occur.92,94,113 Other abnormalities that may be secondary to brachycephalic syndrome include esophageal, gastric, and intestinal inflammation. In one study of 73 dogs with brachycephalic syndrome that underwent endoscopic evaluation of the proximal gastrointestinal tract, common abnormalities included distal esophagitis (37%), gastritis (89%), pyloric mucosal hyperplasia (86%), and diffuse inflammation (53%).92 There are three different stages of laryngeal collapse.90 Stage I is relatively mild, consisting of laryngeal saccule eversion. In stage II, the cuneiform process of the arytenoid cartilage loses its rigidity and becomes medially displaced (Figure 101-7). In stage III, the corniculate processes collapse, resulting in loss of the dorsal arch of the rima glottidis and subsequent airway obstruction.90 Stage II and III laryngeal collapse have been reported in dogs as young as 4.5 months of age.90 Brachycephalic syndrome is most commonly reported in English Bulldogs, pugs, Boston terriers, and Cavalier King Charles spaniels.68,94 Clinical signs include inspiratory stertor (snoring), stridor, coughing, gagging, dyspnea, regurgitation, vomiting, exercise intolerance, and syncope. Diagnosis is based on visual examination of the nares in an awake animal and examination of the palate and larynx under light anesthesia. Thoracic radiographs are recommended in all patients because of the incidence of hypoplastic trachea (38%) and aspiration pneumonia (13.6%) in animals with brachycephalic syndrome.68,94 Because laryngeal collapse represents a secondary condition, the initial treatment is focused on surgical correction of the primary disease and most commonly involves rhinoplasty for stenotic nares (see Chapter 99) and staphylectomy for an elongated soft palate (see Chapter 100). Resection of everted laryngeal saccules is also performed routinely by some surgeons, but others do not believe it improves final outcome.91 In one study, dogs with moderate and severe laryngeal collapse benefited from surgical correction of the primary condition and removal of laryngeal saccules, with life-threatening clinical signs resolved or severely reduced in all cases.113 Snoring or stertor did not resolve completely, however. Laryngeal webbing has been reported after laryngeal sacculectomy.77 Medical management, including weight loss, exercise restriction, and drugs to reduce airway swelling (e.g., glucocorticoids) or edema (e.g., furosemide), can be attempted in animals with signs secondary to persistent laryngeal collapse. Patients that do not respond to surgical and medical management of airway disorders may require permanent tracheostomy. Alternatively, laryngeal tie back may be attempted; however, the effectiveness of this procedure for resolution of airway obstruction has not been extensively evaluated.91 Because gastrointestinal disease is common in dogs with brachycephalic syndrome, some authors recommend treatment with antacid and prokinetic drugs for weeks to months after surgery, particularly if upper digestive tract signs (vomiting, regurgitation, ptyalism) are present.91 In one study, the authors believed that treatment of gastrointestinal disease improved the results of upper airway surgery.91 In that study, medical management was initiated perioperatively, and none of the dogs developed postoperative aspiration pneumonia. The vagus nerve, which originates from the caudal nucleus ambiguus in the medulla, and its branches (the recurrent laryngeal nerves) provide motor function to laryngeal muscles. The recurrent laryngeal nerves eventually terminate as the caudal laryngeal nerves, which have the critical function of stimulating cricoarytenoideus dorsalis muscle contraction and subsequent abduction of the arytenoid cartilages during inspiration. Damage to the nucleus ambiguus, vagus nerve or its branches, or the cricoarytenoideus dorsalis muscle results in laryngeal paralysis. Laryngeal paralysis has been reported in dogs and cats and can be unilateral or bilateral and congenital or acquired. Male dogs are approximately two to three times more affected than female.14,31,71,124 Congenital Laryngeal Paralysis Congenital laryngeal paralysis has been documented in Bouvier des Flandres, bull terriers, Dalmatians, Rottweilers, Pyrenean mountain dogs, and Huskies.* Dalmatians and Huskies are most commonly reported in the United States, and Bouviers and bull terriers in Europe. In Bouviers, the condition is inherited as an autosomal dominant trait.12,115,118 In Siberian Huskies, Husky crosses, and Bouviers, it starts as a progressive degeneration of neurons within the nucleus ambiguus, with subsequent Wallerian degeneration of the laryngeal nerves.8,11,67 The onset of clinical signs in dogs with congenital laryngeal paralysis is usually before 1 year of age. Clinical signs in Bouviers include stridor; pharyngitis; tonsillitis; and, in some dogs, bilateral pelvic limb foot drop from cranial tibial muscle paralysis.67,117,118 Young Rottweilers have been reported with a progressive degenerative disease characterized by neuronal vacuolation and axonal degeneration. Clinical signs include ataxia, paresis, head and muscle tremors, and inspiratory dyspnea.24,67,72 In one report of five Rottweiler puppies, respiratory signs were noted at 11 to 13 weeks of age; all dogs developed tetraparesis, and four of five developed lenticular cataracts. The muscles of the distal limb and larynx underwent neurogenic atrophy, and all dogs were euthanized because of progressive disease.72 Congenital laryngeal paralysis may occur in cats, based on the age at the time of clinical onset in some animals.43,103 Acquired Laryngeal Paralysis: Acquired laryngeal paralysis is most commonly reported in Labrador and Golden retrievers, Saint Bernards, and Irish Setters; the median age of affected animals is 9 years.† The condition has also been reported in cats (mean age, 8.8 years; median age, 11 years).‡ Acquired laryngeal paralysis has been associated with chronic endocrine, infectious, or immune-mediated polyneuropathy.13,33,57,58,67 Most commonly, an underlying cause for polyneuropathy cannot be identified and the condition is considered idiopathic. Other causes include surgical or traumatic damage to the vagus or recurrent laryngeal nerve, lead or organophosphate toxicity, retropharyngeal infection, rabies, polyradiculoneuritis (coonhound paralysis), or laryngeal myopathy.* Dogs with polyneuropathy secondary to hypothyroidism may have concurrent laryngeal paralysis.57,67 On histopathology, these dogs have selective atrophy of type II muscle fibers, a fiber type that is normally fast contracting and easily fatigued.116 Laryngeal paralysis has been diagnosed in cats after bilateral thyroidectomy43,73 and in dogs from stretching or compression of the laryngeal recurrent nerve by a cranial mediastinal or paratracheal mass.61,101 The presenting signs for congenital and acquired forms of laryngeal paralysis are similar. The onset of signs may be acute or chronic; however, unless laryngeal paralysis is a result of trauma or surgery, acute onset in dogs is usually secondary to exacerbation of chronic disease from conditions such as high ambient temperature. Early signs in dogs include a change in voice (phonation) and gagging and coughing, especially during eating or drinking. Gradually, endurance decreases, and exercise intolerance develops. Progression of signs is often slow; months to years may pass before an animal develops severe respiratory distress.37 Often owners think a reduction in exercise is age related or a result of progressive degenerative joint disease. As airway occlusion becomes more severe, laryngeal stridor is noted during inspiration. Severely affected patients have episodes of extreme dyspnea, cyanosis, or syncope.13,37,124 Laryngeal paralysis may be accompanied by various degrees of dysphagia and megaesophagus, which significantly enhances the probability of aspiration after surgical correction of laryngeal paralysis. Patients with unilateral laryngeal paralysis are usually asymptomatic unless they are exercising heavily. In cats, the most common clinical finding is tachypnea or dyspnea.103 Dysphonia, increased upper respiratory noise, inspiratory stridor, exercise intolerance, coughing, dysphagia, weight loss, lethargy, and anorexia have also been reported.43 Because cats and dogs with acquired laryngeal paralysis are old, concurrent disease is common and may result in other clinical signs. In mildly affected dogs, the physical examination is often unremarkable unless systemic signs are present from the underlying disease condition (e.g., polyneuropathy) or from side effects of the condition (e.g., aspiration pneumonia). Dogs may have an inspiratory dyspnea that is not alleviated with open-mouth breathing and that significantly increases with mild lateral compression of the larynx. Because dogs regulate their body temperature with panting, dogs with severe dyspnea from airway obstruction can become hyperthermic. Signs of heat stroke, such as altered mentation, hyperemic mucous membranes, and petechiation, may be present, especially in spring or early summer when ambient temperature is rising. Dogs with heatstroke may be normothermic at presentation. Cats commonly have tachypnea or dyspnea and varying degrees of inspiratory stridor on examination.103 On thoracic auscultation, the animal may have referred upper airway sounds. Harsh crackles, wheezes, or rales may be detected in animals with aspiration pneumonia or pulmonary edema.78 Animals with polyneuropathy may have skeletal muscle atrophy or peripheral neurologic abnormalities, such as decreased postural reactions, spinal reflex deficits, and cranial nerve abnormalities.78 The complete blood count and chemistry profile are usually within normal limits unless concurrent disease is present. An increased white blood cell (WBC) count may be an indicator of aspiration pneumonia. In dogs, the presence of hypercholesterolemia, hyperlipidemia, and increased liver enzymes activity is suggestive of hypothyroidism. A thyroid profile with endogenous thyroid-stimulating hormone and free thyroxine (T4) is required to further define the diagnosis. Severely hyperthermic dogs (body temperature ≥106° F) or those suspected to have heatstroke should undergo additional diagnostics, such as coagulation panels and immediate evaluation of packed cell volume, glucose, and electrolytes and should receive supportive treatment. Heatstroke can progress to disseminated intravascular coagulation, multiorgan failure, and death.78 If myasthenia gravis is suspected, acetylcholine receptor antibody titers are measured. The association of hypothyroidism or myasthenia gravis with laryngeal paralysis is unclear.56,60,71 Thoracic radiographs are performed to rule out other causes of dyspnea (e.g., lung lobe tumors); detect underlying etiologies (e.g., cranial mediastinal masses); and look for concurrent pathology such as aspiration pneumonia, noncardiogenic pulmonary edema, or megaesophagus. Aspiration pneumonia has been reported in 7.9% of dogs with laryngeal paralysis.71 If aspiration pneumonia is present, surgical intervention should be delayed until the aspiration pneumonia is resolved because it increases the risk of postoperative complications.71 Patients with pulmonary edema from airway obstruction may require immediate surgery to enlarge the laryngeal ostium or bypass the obstruction. In cats, the most common radiographic changes are associated with airway obstruction, including hyperinflation of the lungs; caudal displacement of the larynx; and air in the pharynx, larynx, esophagus, and stomach. In one report of cats with laryngeal paralysis, 2 of 15 cats had megaesophagus, and 1 of 15 cats had evidence of aspiration pneumonia on plain radiographs.103 Megaesophagus may be present in dogs with laryngeal paralysis, especially if the condition is secondary to polyneuropathy or polymyopathy. In one study, preoperative esophageal disease was diagnosed in 11.4% of dogs with laryngeal paralysis and was associated with increased risk of postoperative complications.71 Esophageal dysfunction may not be evident on plain films but may be detected on esophagrams. In one study, dogs with idiopathic laryngeal paralysis had significant esophageal dysfunction compared with age- and breed-matched control subjects.108 Dysfunction was more pronounced in the cervical and cranial thoracic esophagus. Dogs that developed aspiration pneumonia also had significantly worse esophageal function than those that did not.108 Esophagrams are not routinely performed by most clinicians because of the risk of aspiration in affected patients. Ultrasonography has been used to evaluate the larynx and laryngeal function. In one study, 30 of 30 dogs with laryngeal paralysis had asymmetry or absence of motion of the cuneiform processes on ultrasonographic evaluation.99 Other findings included abnormal arytenoid movement (16 of 30), paradoxical motion (9 of 30), caudal displacement of the larynx (2 of 30), and laryngeal collapse (1 of 30). In another study, ultrasonography was not as effective as direct observation of the larynx for diagnosis of laryngeal paralysis.93 Laryngeal paralysis is definitively diagnosed by laryngeal examination under a light plane of anesthesia.* The animal should be anesthetized to the point at which the mouth can be easily opened but a laryngeal reflex is still present. If the animal is too deeply anesthetized, even a normal larynx may appear paralyzed; affected animals should be allowed to approach consciousness during examination if this occurs. The animal should be placed in sternal recumbency and the head elevated to a normal level of carriage. A videoendoscope is useful for examination because it is less likely to require ventral epiglottic retraction, which is often necessary for laryngeal visualization when a hand-held laryngoscope is used. During laryngoscopy, SPO2 should be monitored, and flow-by oxygen can be administered through a tube attached to the laryngoscope blade or videoendoscope instrument port. In a normal animal, vocal folds and arytenoids should abduct during inspiration and passively relax during expiration. A gap remains between the arytenoids at rest. In animals with laryngeal paralysis, arytenoid cartilages and vocal folds are immobile or drawn toward the midline during inspiration. If only one arytenoid abducts, paralysis is unilateral. A gap also remains between the arytenoids at rest in animals with laryngeal paralysis; however, the gap may be narrower if laryngeal edema is present. Edema and erythema of the arytenoid cartilage mucosa are usually present on the dorsal part of the larynx and appear to result from repeated trauma from the arytenoids hitting each other at each inspiration.31,37,55,62,79
Larynx
Anatomy
Feline Anatomy
Physiology
Laryngeal Neoplasia
Treatment
Partial Laryngectomy
Total Laryngectomy
Laryngeal Collapse
Treatment
Laryngeal Paralysis
Etiology
Clinical Findings
Laboratory Findings
Diagnostic Imaging
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


