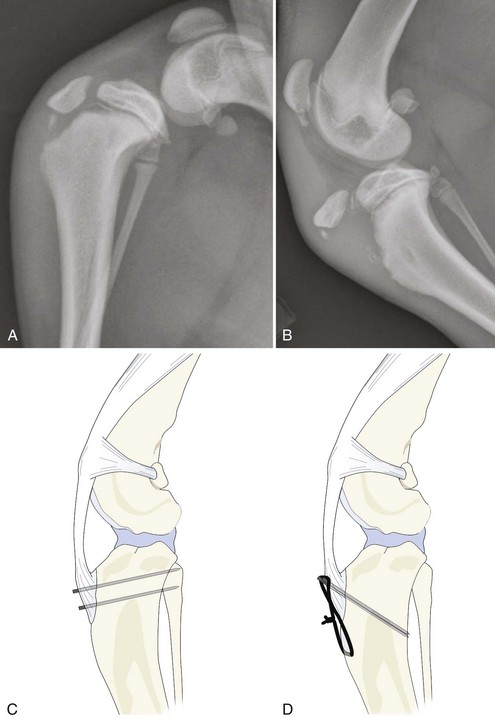
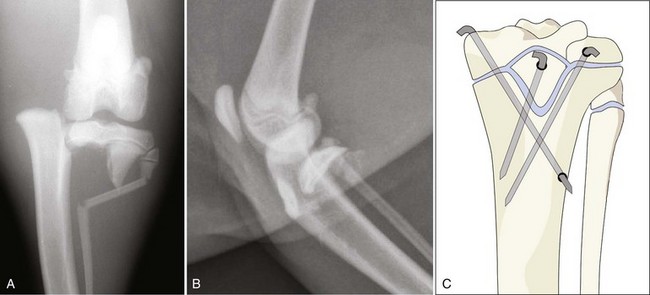
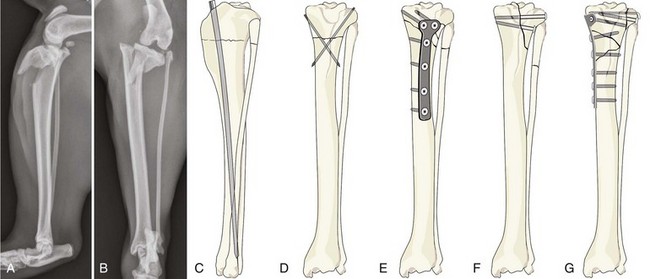
Chapter 63 Fractures of the tibia are relatively common in dogs and cats, accounting for 10% to 20% of all fractures.5,6,40 Tibia fractures often result from trauma, and approximately 50% of tibia fractures occur in young dogs and cats.5,6,40 A majority of tibia fractures are diaphyseal fractures. Ten percent to 20% of all tibia fractures are open fractures, with the distal tibia of mature animals being the most common site of an open fracture. Immediate immobilization of the crus is recommended and surgical treatment is often indicated for fracture of the tibia. A variety of repair methods can be applied for tibial fracture, and selection of a repair procedure depends on multiple factors, including the type and location of the fracture, the age of the animal, the presence of associated soft tissue defects and infection (particularly in open fractures), economic considerations, and the surgeon’s preference. Concurrent fracture of the fibula is common, although repair of the fibula generally is not indicated unless the proximal fibula or the lateral malleolus is involved.29 The overall prognosis following fracture of the tibia and fibula is generally good when appropriate treatment is applied. The tibia is a long bone that is crucial for locomotive function of dogs and cats. The tibia articulates with the femur proximally, with the tarsus distally, and with the fibula on its lateral side both proximally and distally. The tibia serves as an attachment site for many muscles, including the quadriceps femoris (stifle joint extensor), the biceps femoris, and the caudal part of the sartorius (stifle joint flexor) and cranial tibial (tarsal flexor) muscles.12 The fibula is a thin bone that contributes little to weight bearing in dogs and cats. The fibula articulates with the caudolateral part of the lateral condyle of the tibia proximally, and with the tibia and the talus distally. The fibula serves as an attachment site for a few muscles and for collateral ligaments of the stifle and the tarsal joints. Wide variation in the length and shape of the tibia and fibula is seen among breeds. A method for radiographic measurement of the bony axis of the tibia has been described recently in dogs.8 The tibia has four separate epiphyses: proximal epiphysis, tibial tuberosity epiphysis, distal epiphysis, and medial malleolar epiphysis (Figures 63-1 and 63-2).37 The proximal epiphysis is relatively flat and forms the articular surface of the tibia. The proximal epiphysis sits on the metaphysis, and the interface between epiphysis and metaphysis contains two small concavities that help to interdigitate the epiphysis to the metaphysis.27 The associated physis (growth plate) is responsible for approximately 40% of the length of the tibia.19 The tibial tuberosity is a traction epiphysis (apophysis) that forms the prominence to which the patellar ligament attaches. It has a histologically identifiable physis, although growth occurs at a slower rate than in the nearby proximal epiphyseal plate, and it does not contribute substantially to the length of the bone.16 At some point in development (between 6 and 8 months in large-breed dogs), the proximal epiphysis fuses to the tibial tuberosity epiphysis (apophysis).27,41 The apophyseal growth plate has a flat interface with the metaphysis. The apophyseal growth plate normally closes relatively late in the development of the dog (>12 months in large-breed dogs).41 Premature closure of the associated growth plate may cause tibial deformity.13,29,31 The distal tibial epiphysis interfaces with the metaphysis via two triangular convexities in the metaphysis and corresponding concavities in the epiphysis.27 The growth plate is responsible for approximately 60% of longitudinal growth of the tibia.19 The epiphysis of the medial malleolus fuses to the distal tibial epiphysis very early in development (4 to 5 months in large-breed dogs).37 This epiphysis may not always be identifiable (see Figure 63-2). The fibula has two epiphyses: one proximal epiphysis and one distal (see Figures 63-1 and 63-2). The distal epiphysis contributes to the lateral malleolus (see Figure 63-2). These epiphyses are mainly responsible for diaphyseal length. The proximal end of the tibia is relatively flat and triangular and is formed by two flat condyles that make up the tibial plateau, which articulates with the femoral condyles.12,27 Although the tibial plateau is broad, the articular surface is relegated to the caudal one half of the proximal tibia.12,27 The cranial portion of the tibial plateau occupies the area associated with the stifle fat pad. The tibial tuberosity is located just distal to the cranial border of the tibial plateau. The tibial tuberosity is the quadrangular proximocranial process that provides insertion for the quadriceps femoris muscle via the patellar ligament and parts of the biceps femoris and sartorius muscles. The tuberosity continues distally as the cranial border of the tibia (formerly called the tibial crest) and tapers to join the diaphysis. The tibial body is three-sided proximally (medial, lateral, and caudal surfaces), whereas the distal half is essentially cylindrical, and the entire medial part of the distal extremity of the tibia forms the medial malleolus. The proximal tibial metaphysis is relatively flat medially but is concave both laterally and caudally. All these surfaces blend into the tibial diaphysis, which is uniform in diameter but slightly S-shaped.27 It curves from medial to lateral in the proximal one half and then from lateral to medial in the distal one half.27 The distal part of the tibia is flared slightly and forms the distal articular surface and the medial malleolus. The medial malleolus is the proximal attachment of the medial collateral ligament of the talocrural joint. The fibula is divided into a head (proximal extremity), body (or shaft), and lateral malleolus (distal extremity). The fibula is a very thin bone. Its proximal end is enlarged to form the fibular head, which serves as the distal attachment of the lateral collateral ligament of the stifle joint. The fibular diaphysis is very thin and possesses a very small or no medullary cavity.27 Distally, the diaphysis enlarges to form the lateral malleolus, which serves as the proximal attachment of the lateral collateral ligament of the tarsus. The fibula and collateral ligaments, together with the tibiofibular ligaments, contribute to tarsal stability. The tibia receives its blood supply from the nutrient artery and the periosteal vessels derived from the cranial tibial artery.12 The nutrient foramen is located in the caudolateral edge of the proximal one third of the diaphysis. Within the medullary canal, the nutrient artery divides into proximal and distal branches that anastomose with the metaphyseal arteries at each end.19 These anastomoses permit the metaphyseal arteries to sustain the medullary arterial supply when the principal nutrient artery is disrupted by fracture or surgery.19 The medullary arteries supply the inner two thirds of the tibial cortical circulation, whereas the periosteal arteries supply the outer one third of the cortical circulation.19 The fibular head is supplied by a branch of the cranial tibial artery, and the fibular body is supplied by the nutrient artery derived from the peroneal artery. The cranial branch of the medial saphenous artery and vein and the saphenous nerve pass obliquely across the diaphysis of the tibia.28 Arteries (such as the tibial and popliteal arteries) and nerves (such as the peroneal and cutaneous nerves) run along the lateral and caudal aspects of the tibia and fibula; fortunately, surgical approaches in these areas are rarely required. The anatomy of the tibia and fibula in cats is similar to that in dogs. The medullary cavity of the feline tibia appears to be more uniform in diameter than in dogs, but no other substantial difference has been noted.27 Fractures of the tibia and fibula account for approximately 20% of long-bone fractures and 10% of all fractures.5,6,22,40 The tibia/fibula is the fourth most common fracture location in dogs after the pelvis, femur, and radius/ulna.22 Although not specified for all cases in the study, trauma appears to be the most common cause of the tibial/fibular fracture, with automobile-related trauma accounting for approximately 50% of fracture cases. Left and right sides and male and female animals are equally affected.5,6,40 Boone reported that slightly more than 50% of tibial fractures occurred in dogs and cats <1 year of age.5,6 Open fractures and comminuted fractures occurred more frequently in animals older than 1 year. Open fractures accounted for 12% of diaphyseal fractures and 37% of distal fractures in these studies.5,6 Diaphyseal fractures are significantly more common than fractures of the proximal and distal regions of the tibia.5,6,40 Proximal, diaphyseal, and distal fractures accounted for approximately 1%, 83%, and 18% of fractures in two studies by Boone (multiple locations involved in some fractures), and for 7%, 72%, and 20% of fractures in a study by Unger.5,6,40 Studies by Boone also reported that 100% of proximal fractures, 55% of diaphyseal fractures, and 41% of distal fractures occurred in animals younger than 1 year of age.5,6 Tibial tuberosity avulsion and physeal fracture are the two most common types of proximal fracture.5,6,40 Unger reported that nonarticular (Salter-Harris type I or II) fractures were the most common type and accounted for 56% of proximal fractures.40 Fractures involving the articular surface were rare and accounted for only 2% of proximal fractures.40 The mid-diaphysis is the most common location of diaphyseal fracture (64%) compared with proximal (20%) and distal (15%) diaphyseal fractures.6 Oblique/spiral fractures and comminuted fractures appear to be the most common fracture patterns.6,40 Boone reported that diaphyseal fractures included incomplete (5%), transverse (14%), oblique/spiral (44%), comminuted (34%), and segmental fractures (3%), and Unger reported that diaphyseal fractures included incomplete tibia or fibula intact (19%), transverse (6%), oblique/spiral (21%), comminuted (53%), and segmental fractures (1%).6,40 Physeal fractures and fractures of the medial or lateral malleolus are the two most common types of distal fractures.5,40 Boone reported that distal fractures included physeal (31%), malleolar (58%), and metaphyseal (9%) fractures.5 A majority of the physeal fractures were Salter-Harris type I or II. Medial and lateral malleoli were equally affected.5,40 Unger reported that distal fractures included simple nonarticular fractures (including physeal fractures) (60%) and malleolar (28%) fractures.40 Nonmalleolar articular fractures were very rare and accounted for only 0.2% of distal fractures. The entire spectrum of internal and external fixation devices is applicable to tibial fracture.29 Biologic factors (such as age and health of the patient, blood supply and soft tissue damage, and location of the fracture), mechanical factors (such as type and stability of the fracture, size and activity of the patient, and the number of limbs injured), and clinical and practical factors (such as financial constraints, patient and client compliance, and the surgeon’s preference and experience) should be considered to determine an appropriate plan for successful fracture management. Fractures of the proximal region of the tibia generally involve the physis in young animals (Figures 63-3 and 63-4) and the metaphysis in mature animals (Figure 63-5). Most fractures are simple, and multifragmentary or articular types are rare. The surgical approach to the medial side is achieved by skin incision directly over the area of interest.28 Exposure of the lateral aspect of the proximal tibia involves elevation of the cranial tibial muscle. Care is taken not to damage the tendon of origin of the long digital extensor muscle during elevation of the cranial tibial muscle. Arthrotomy of the stifle joint can be added when indicated but is rarely necessary. Avulsion of the Tibial Tuberosity Avulsion of the tibial tuberosity (see Figure 63-3) occurs relatively infrequently and is limited to younger animals, usually between 4 and 8 months of age.29 The tuberosity is an apophysis that fuses to the proximal epiphysis and then to the metaphysis of the tibia as the animal reaches skeletal maturity (see Figure 63-1). In large dogs, the growth plate associated with the tuberosity closes late in development; thus the endochondral ossification process of the physis may seem irregular radiographically and may be mistaken for a pathologic process.41 The tibial tuberosity serves as the insertion site of the quadriceps femoris muscle, and avulsion of the tuberosity can result from contraction of the muscle while the stifle joint is flexed and the foot is set firmly on the ground.29 Clinically, lameness, pain, stifle joint effusion, and soft tissue swelling are noted. The proximally displaced avulsed tuberosity may be palpable. Avulsion of the tibial tuberosity is best demonstrated on a lateral radiograph, especially when the leg is flexed (see Figure 63-3). Care should be taken to avoid mistaking the normally wide growth plate in the immature animal for a fracture; therefore, radiographs of the opposite limb should be taken for comparison. Varying degrees of avulsion may be seen, from minimal displacement to complete detachment.13,29,31,41 Treatment options should be determined based on the degree of displacement, the size of the animal, and the remaining growth potential (age). Conservative management with external coaptation (cast or splint) should be considered only when the displacement is minimal and the patient is a small-breed dog. External coaptation should be maintained for 2 to 3 weeks. In most cases, open reduction and internal fixation is recommended. Many different techniques have been described for repair of this fracture, including use of pins alone or pins and tension band wire.29 The avulsed tibial tuberosity is usually located proximal to the fracture site. The displaced tuberosity is reduced by placing a hook or pointed bone reduction forceps over the proximal portion of the tuberosity, and by carefully pulling the tuberosity back into position with the hip flexed and the stifle joint extended. Care is taken in young animals with soft bone when using bone forceps, as the tuberosity can fragment easily. Fixation with two Kirschner wires alone (without tension band wire) is recommended only for very young small dogs with less than total avulsion. If pins are used as the sole method of repair, they should be inserted in a caudoproximal direction to counteract the considerable pull of the quadriceps mechanism (see Figure 63-3, C). Pin and tension band wire fixation is the preferred technique for repair (see Figure 63-3, D).29 If the avulsed part of the tuberosity is very small, reattachment of the patellar ligament to the tibia can be achieved by placement of tendon sutures through the ligament and through a transverse bone tunnel(s) in the tibial body.29 Strict exercise restriction is recommended for 1 to 2 weeks, followed by progressive limited leash walking over 2 to 3 weeks. Short-term application of a soft-padded bandage may be indicated. Clinical and radiographic examination should be performed at 4 to 6 weeks postoperatively. If the animal has a considerable amount of growth potential remaining (large and medium breeds <6 months old, and small breeds <4 months old), the fixation should be removed as early as possible (when clinical and radiographic union is achieved) to avoid premature fusion of the tuberosity to the shaft and eventual distal translocation of the tuberosity.29 Fixation complications include avulsion of the tuberosity from the implant, wire or pin breakage, bending of a pin, pin migration, entry of a pin into the proximal epiphysis, and deformity of the proximal tibia.13,31 Premature closure of the apophyseal growth plate and deformity of the tibial tuberosity are common; however, the prognosis for normal function is generally good. Fractures of the proximal physis of the tibia (see Figure 63-4) are usually Salter-Harris type I or II fractures in young animals.40 The combined proximal epiphysis and tibial tuberosity are usually involved, and the tibial metaphysis/diaphysis is frequently displaced in a craniomedial direction.29 Occasionally, the proximal epiphysis is separated from the tuberosity, and this may be accompanied by collateral ligament damage.29 Clinically, lameness, pain, stifle joint effusion, and soft tissue swelling are noted. Closed reduction and application of external coaptation is indicated only in cases with minimal displacement. A lateral splint bandage can be applied for 2 to 3 weeks. In most cases, an open approach is necessary to reduce the epiphysis to its proper position.29 A craniomedial or craniolateral approach is used over the stifle joint and the proximal tibia.28 Reflection of the cranial tibial muscle may assist in exposing the fracture to achieve reduction and fixation.29 If the fibula is fractured and overriding, its reduction may be helpful in supporting and restoring length to the lateral surface of the tibia.29 During reduction, care should be taken not to disturb the growth plate. The fracture can be reduced by pulling the tibial metaphysis laterally to realign it under the epiphysis. In some cases, gentle levering of the epiphysis onto the metaphysis may be necessary. Repair using multiple Kirschner wires or small pins is the easiest and most versatile fixation method (see Figure 63-4, C).29 Pins are passed through the nonarticular portions of the medial and lateral edges of the epiphysis and are crossed in the metaphyseal portion of the tibia. One pin placed medially and one placed laterally may be adequate; however, a third fixation point in the tibial tuberosity is recommended for better stability.29 In some Salter-Harris type II fractures that have a large metaphyseal portion (see Figure 63-4, A), insertion of one or two interfragmentary screws may be indicated (see Figure 63-5, F).29
Fractures of the Tibia and Fibula
Anatomy
Developmental Anatomy
Anatomy of Mature Dogs and Cats
Fracture Epidemiology
Proximal Fractures
Diaphyseal Fractures
Distal Fractures
Preoperative Management
Proximal Fractures
Immature Animals
Physeal Fractures
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Fractures of the Tibia and Fibula


Only gold members can continue reading. Log In or Register to continue
