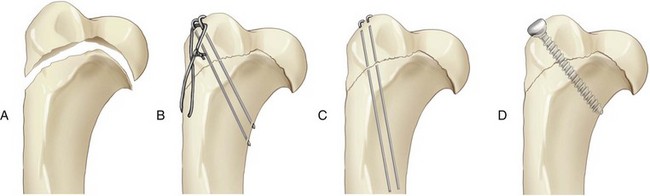
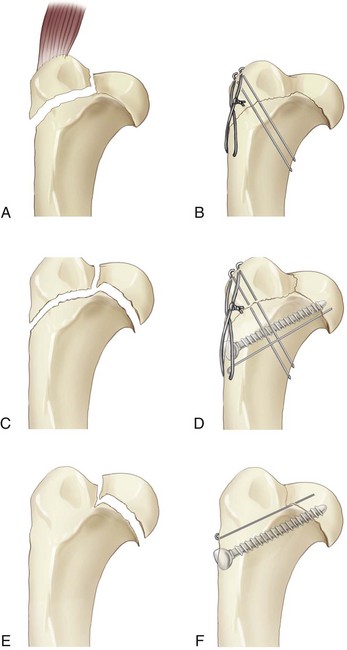
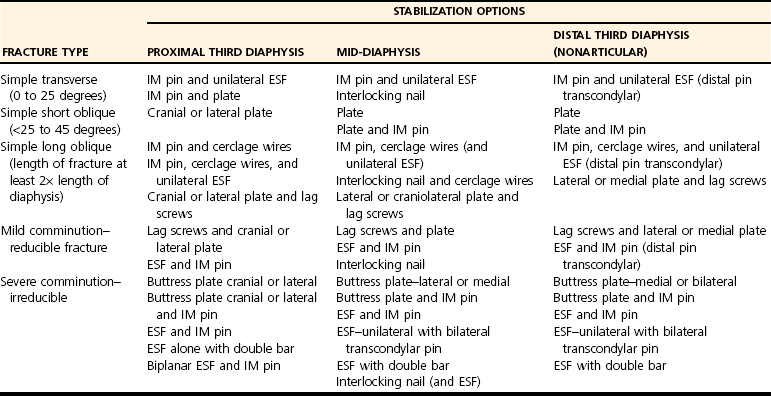
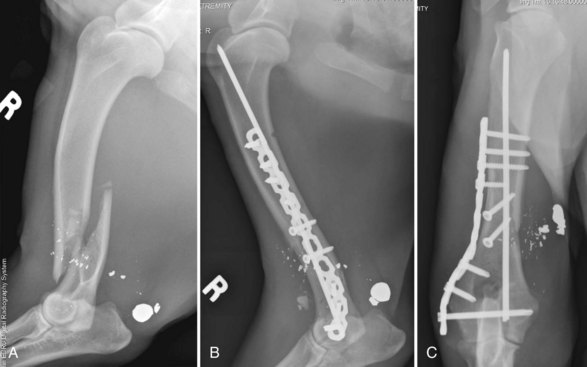
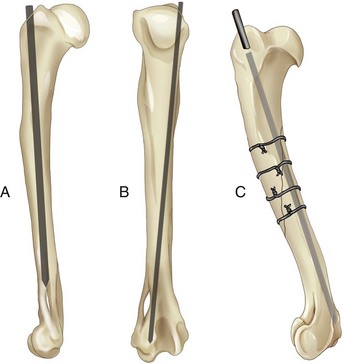
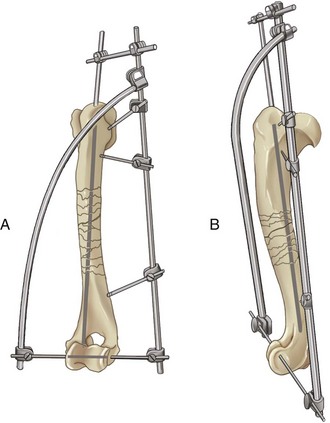
Chapter 52 Humeral fractures account for 8% to 10% of fractures in dogs and 5% to 13% of fractures in cats.37,42,63,68 Diaphyseal humeral fractures are caused by road traffic accidents, gunshots, and falls; distal fractures are caused mainly by falls or jumps.5,90 Most humeral fractures involve the middle and distal one third of the bone.34 The humerus is a difficult bone to surgically approach and repair because of its shape, location, and surrounding anatomic structures. It is an upper limb bone with a large surrounding muscle mass, it is an S-shaped bone with a twist, and ridges proximally and distally make accurate plate contouring difficult. The radial nerve crosses the distolateral aspect, and the median and ulnar nerves run on the medial aspect. In the cat, the median nerve and a branch of the brachial artery pass through the supracondylar foramen (Figure 52-1). The distal third of the shaft in the dog and cat is compressed in a craniocaudal direction, and this dense cortical bone with its close association with the radius and ulna is prone to shattering and fissuring. Additionally, the medullary canal tapers and effectively ends far proximal to the distal aspect of the bone, limiting intramedullary pin purchase in the condyle of the humerus, and thereby compromising the stability of fracture repair when that method of treatment is used.49 Figure 52-1 The humeral supracondylar foramen in the cat through which the median nerve and brachial artery pass. Because of the location of the humerus in relation to the vital structures of the head and thorax, a careful evaluation of the patient with a humeral fracture should be performed before further investigation and surgery. A large number of animals with humeral fractures have concurrent thoracic, abdominal, or skull injuries.48,80,81 Most patients with a humeral fracture carry the leg with the affected elbow dropped and with the paw resting on its dorsal surface because of pain and weakness in the extensor musculature. This mimics the appearance of loss of proprioception resulting from nerve injury.69 It is important before surgery to ascertain that the nerve supply to the leg is intact; radial nerve injury or a brachial plexus or spinal nerve root avulsion can occur concurrent with humeral fracture. Physical examination tests such as toe pinch and skin prick should be performed; the presence of Horner’s syndrome or loss of the panniculus reflex together with neurologic deficits in the forelimb would be indicative of a brachial plexus injury. Nerve conduction studies are helpful only approximately 7 days after the injury occurs.30 If cutaneous sensation is present in the affected leg, motor function is usually regained within 1 to 6 weeks in most animals.87 The humerus is an important bone for transfer of weight and for propelling the body forward; by its position, it also provides a protective function for the thorax. The humeral head articulates proximally with the scapula, and the humeral condyle articulates distally with the radius and ulna. The head of the humerus is on the caudal aspect of the bone. The bigger and most craniolateral proximal protuberance is the greater tubercle, which is separated by the intertubercular groove from a small, indistinct lesser tubercle. The tendon of origin of the biceps brachii muscle runs in the intertubercular groove and is held in place by the transverse humeral ligament. A bony ridge, the tricipital line, extends from the humeral head cranially and distally toward the deltoid tuberosity, and it is the site of origin of the lateral head of the triceps brachii muscle. The bone cranial and proximal to this line is generally cancellous with a relatively thin cortex; more caudally, the cortical bone thickens, and this is important in terms of improved implant holding power.61 Cranial and distal to the tricipital line is the deltoid tuberosity, at the level of the proximal and middle thirds of the humerus; it is the insertion point for the deltoideus muscle. The humerus tapers and narrows from proximal to distal, which has implications when intramedullary implant sizes are selected. The humerus also has an S shape, which is more pronounced in the dog than in the cat and is particularly accentuated in chondrodystrophic breeds such as Dachshunds. From proximal to distal, the bone curves cranially from the humeral head to caudally along the diaphysis, and then cranially again at the condyle. This shape can cause difficulty when bone plates are selected and contoured. From the deltoid tuberosity, the humeral crest spirals distally toward the lateral epicondyle; the cranial border of the brachialis muscle courses along the crest. The most distal end of the humerus is referred to as the humeral condyle. The medial side of the condyle—the trochlea—articulates with the trochlear notch of the ulna. The smaller, laterally located part of the humeral condyle is the capitulum. The capitulum articulates with the radial head. The medial and lateral sides of the condyle have epicondyles, which are eminences, or projections, on the surface of the condyle that serve as an area of attachment for ligaments and tendons. The lateral and medial collateral ligaments originate from the lateral and medial epicondyles, respectively. The lateral epicondylar crest extends proximally from the lateral epicondyle to blend with the humeral shaft. 24 Cranial and proximal to the condyle is the shallow radial fossa, which communicates via the supratrochlear foramen with the caudal deeper olecranon fossa.9 In the dog the supratrochlear foramen is closed off in life by a membrane. In the cat, a supracondylar foramen is located proximal to the medial epicondyle, and a true supratrochlear foramen is absent. The median nerve and the brachial artery pass through the supracondylar foramen before continuing into the antebrachium and distal limb. In the cat, communication between the olecranon fossa caudally and the radial fossa cranially is interrupted by bone across the supratrochlear “foramen.” The nerves that supply the brachium originate at the brachial plexus. Major nerves encountered during surgical approaches to the humerus are the median and ulna nerves medially and the radial nerve laterally. The radial nerve originates proximomedial to the humerus, passing deep to the lateral head of the triceps brachii muscle while branches supply the heads of the triceps brachii muscle. The nerve continues to course distally and cranially alongside the brachialis muscle, giving off branches that innervate the digital and carpal extensor muscles and the extensor carpi ulnaris (ulnaris lateralis) muscle. Among the nerves of the thoracic limb, the radial nerve, with its lateral position in the region of the distal humerus, is the most vulnerable to damage from the initial trauma associated with fracture of this region of the humerus. The radial nerve is also susceptible to iatrogenic damage during a craniolateral approach to the distal shaft of the humerus.70 Fractures of the humerus in the dog are most likely to affect the distal part of the bone. By comparison, fractures in the cat are more likely to affect the mid-diaphysis, and fractures in the condylar region are less common (Table 52-1). In this chapter, fractures of the humerus will be discussed, from those affecting the proximal region of the bone to those affecting the most distal region. Mention will be made of the types of fractures that occur and their pathogenesis, along with appropriate surgical approaches and techniques that can be used to stabilize fractures and the complications that are most likely to occur. Table • 52-1 Percentage of Fractures Occurring in Each Part of the Humerus in the Dog and Cat5 Fractures of the proximal humerus include physeal and metaphyseal fractures. Fractures of this region occur infrequently because of the large cross-sectional area of the bone and its close proximity to the body.88 The most common fractures of this region are physeal fractures in immature animals. The occasional simple or comminuted fracture is seen in the metaphyseal area in adult dogs, often as a result of direct trauma such as gunshot, or pathologic fracture due to inherent bone weakness induced by neoplasia or systemic disease. The proximal humeral physis is a complex entity. The capital center of ossification appears first, at between 14 and 16 days, and slowly invades the cranial aspect of the epiphysis to form the greater tubercle at around 4 months. The whole epiphysis fuses with the metaphysis between 7.5 and 12 months in the dog,79,86 and between 19 and 26 months in the cat.84 The humeral head and the greater tubercle fuse at an angle of approximately 102 degrees in the dog,64 to form the epiphysis that sits like a “cap” on the metaphysis and has inherent stability after fracture reduction. Salter-Harris type I and II76 fractures affect the humeral head; these are usually seen in young dogs or cats before physeal closure. The humeral head or the greater tubercle can separate independently, or, more commonly, the two epiphyses can stay confluent. When fracture occurs, the humerus is usually displaced caudal and lateral to the physis. All proximal humeral physeal fractures are exposed via a combined approach to the craniolateral region of the shoulder joint and the proximal humerus,70 with little additional dissection required because the tissue planes are usually adequately separated at the time of injury.64 The fracture can be reduced by gentle leverage using a Hohmann retractor, while traction is applied through bone-holding forceps applied to the distal fragment. Placing the shoulder in extension often assists fracture reduction.88 Care must be taken to ensure accurate fracture reduction in all planes. For Salter-Harris type I or II fractures, when the two fragments (the humeral head and the greater tubercle) are still together, stabilization can be achieved by placing two pins from the proximal aspect of the greater tubercle into the humeral neck or the proximal diaphysis (Figure 52-2). In young animals with potential for further growth, it is preferable to place the Kirschner wires in a parallel fashion so as to minimize compression of the growth plate and allow for continued physeal growth. In animals at or near skeletal maturity, a wider variety of fixation devices, including lag screws and tension band wires, can be used to provide additional stability (Figure 52-3).69 Rarely, the greater tubercle and/or the humeral head fracture separately.16 The greater tubercle is subjected to tensile forces from the supraspinatus muscle during the swing phase of the gait cycle; in addition, the tubercle lies lateral to the shoulder joint, making it vulnerable to trauma. Both of these features predispose the greater tubercle to avulsion fracture.16 If the humeral head is separate from the greater tubercle, then both bony fragments are repaired with small Steinmann pins or Kirschner wires (see Figure 52-3). Kirschner wires used to secure the humeral head are placed from cranial to caudal, with the pins inserted just distal to the greater tubercle and directed slightly proximally and caudally; care is taken that the pins do not penetrate the articular surface. Rarely, the humeral head can separate in isolation; this was reported in a 4-year-old Dachshund.38 The injury can be repaired with Kirschner wires alone or with a lag screw. The very infrequent fracture of the lesser tubercle can be treated via a craniomedial approach to the shoulder with reflection of the proximal attachment of the pectoral musculature.70 The fragment can be secured using crossed Kirschner wires or a small lag screw. No external coaptation should be necessary following stabilization of fractures of the proximal humeral physis, although exercise should be restricted for at least 4 weeks. The prognosis is very good for complication-free healing.5 The metaphyseal region of the proximal humerus is an area prone to fracture when the bone is weakened or osteoporotic, for example, in young dogs and cats with nutritional secondary hyperparathyroidism or in older animals when the bone has been weakened by neoplasia. Fractures are often of a transverse impaction type18 and therefore are relatively stable. If the underlying metabolic disease is corrected, the fracture will usually heal, but malunion may result. The proximal metaphysis is an area of predisposition for primary bone tumors, most commonly, osteosarcoma. Pathologic fracture secondary to osteosarcoma is not unusual, and radiographic changes typical of a primary bone tumor are usually evident. Iatrogenic fracture of the proximal humerus can occur through cortical defects made for harvesting cancellous autograft.25 These usually spiral fractures extend distally into the humeral diaphysis from the hole in the proximal bone. Because only a small proximal fragment is present, stabilizing these fractures can be a challenge.61 A variety of diaphyseal humeral fractures are recognized in dogs and cats, ranging from simple transverse, spiral, and oblique fractures to the more complicated and challenging comminuted fractures. Diaphyseal humeral fractures are most commonly the result of road traffic accidents, falls, or kicks.5 Surgical approaches to the humerus are technically demanding because of important neurovascular structures on the lateral and medial aspects of the bone, and the large amount of surrounding musculature.93 These approaches are described in detail in other textbooks.70 The approach to the craniolateral aspect of the humerus, combined with the approach to the proximal humerus, will expose the proximal three quarters of the humerus.69 The triceps brachii muscle is reflected caudally, and the biceps brachii, pectoral, and brachiocephalicus muscles are retracted cranially. The radial nerve with the brachialis muscle can be reflected cranially or caudally according to the position of the fracture. The medial approach to the humerus involves cutting the pectoral muscle origins proximally, reflecting the biceps brachii muscle caudally and the brachiocephalicus muscle cranially. If exposure needs to be continued in a more distal direction, the biceps brachii muscle can be reflected cranially. Great care must be taken to identify the median and ulnar nerves and the brachial vessels when a medial approach is taken. Various fixation methods can be used effectively for humeral fracture stabilization.8 Closed or open intramedullary pinning, external skeletal fixation, interlocking nail, bone plates and screws, or combinations of these techniques have been used successfully to repair diaphyseal humeral fractures.* When the decision is made as how to best stabilize a diaphyseal fracture, the final choice is dictated and influenced by many factors, including type of fracture, the patient’s age, nature and size of the animal, surgeon’s experience, implants available, and expense of the procedure. Ultimately, the aim should be to achieve uncomplicated fracture healing and return the animal to soundness and full function as soon as possible. Fracture repair of the humerus is challenging because of the high forces placed on fracture fragments, particularly with fractures close to the elbow. In the distal bone, relatively little bone stock is present, and it is often of a brittle nature. Optimizing the number of implants that can be placed in small fracture fragments and achieving a stable fracture repair should be the main goals of the surgeon. Diaphyseal fractures can be divided according to location affected (proximal, middle, and distal) and degree of comminution. Fractures of the distal diaphysis do not communicate with the supratrochlear foramen (fractures entering the supratrochlear foramen are classified as supracondylar fractures). Considerable overriding of fragments, due to contraction of the brachial muscles, often occurs. Open reduction is often necessary to reduce these fractures. Some options for fracture repair are listed in Table 52-2 with the obvious provisos as mentioned previously. In severely comminuted long bone fractures where anatomic reconstruction is not possible or is of questionable benefit, a biologic strategy of stabilizing the proximal and distal fragments, maintaining limb and joint alignment, and not interfering with the blood supply to the fragments can be adopted. In the following sections, various implants systems will be discussed specifically in relation to their use for stabilization of humeral fractures. More detailed information on internal and external stabilization of fractures in general is provided in Chapters 43 and 44. Fractures of the humerus are rarely suitable for external coaptation because of the difficulty involved in immobilizing the proximal limb joints. A spica splint is the only device that will give some stability to the shoulder and elbow.69 Few indications are known for nonsurgical management of humeral fractures in the dog and cat because these fractures are usually displaced and unstable. A minimally displaced fracture of the proximal physis or a greenstick fracture in a young puppy or kitten would be a possible indication for this form of fixation.69 If nonsurgical treatment is chosen for unstable fractures, owners should be aware that the outcome may be less than ideal; possible complications include limb shortening, malunion, nonunion, and ankylosis.81 Intramedullary pins are readily available and relatively inexpensive implants that are often used in combination with other devices for humeral fracture stabilization.39 In one report that described 130 humeral fractures, 30% were repaired with an intramedullary pin or an intramedullary pin–containing construct.5 Because of proximity to the neutral axis, the intramedullary pin resists bending well in all directions,83 but the implant has limitations, namely, the inability of the pin to resist the deleterious forces of rotation, shear, and axial compression.3 The intramedullary pin in the humerus is usually used in combination with cerclage wires when the fracture is long oblique and simple, with external skeletal fixation to prevent rotation or collapse for simple transverse or comminuted fractures, and in combination with plate fixation for comminuted fractures. Cerclage wires must be used with caution in the humeral diaphysis because the tapered shape of the diaphysis tends to cause the wire to move distally when placed on the proximal portion of the shaft and proximally when placed on the distal portion of the shaft.88 When an intramedullary pin is combined with a plate, the pin can help align fracture fragments, prevent bending forces, and reduce the stress applied to the more abaxially placed bone plate (Figure 52-4).40 Forty-seven cases, including nine humeral fractures, treated with a plate rod (intramedullary pin) construct and principles of biologic osteosynthesis, were reported by Reems and others72; fracture healing was successful in 46 of the 47 cases. Investigators recommended using a pin that measures 35% to 50% of the diameter of the medullary canal, in combination with the plate. Goals were that the pin should provide some stability, should reduce the chance of plate failure, and should allow adequate room for placement of some bicortical screws.72 When intramedullary pins are inserted in dogs, it is recommended that the pin is angled toward or inserted into the medial aspect (trochlea) of the humeral condyle to increase bone purchase and length of the pin used. Therefore, the size of the pin selected should allow it to pass through the medial epicondylar crest into the medial aspect of the condyle.69 When an intramedullary pin is used in cats, where the intramedullary canal of the medial epicondylar crest is rarely wide enough to allow passage of a pin into the medial aspect of the condyle, it is preferable to direct the pin into the central area of the distal diaphysis just proximal to the olecranon fossa (Figure 52-5).47 Use of an intramedullary pin in this manner should be restricted to fractures of the proximal half of the diaphysis because anchorage of the pin is not firm in the distal fragment.69 In most dogs and in some large cats, it may be possible to insert a small pin into the medial aspect of the condyle (see Figure 52-5). Open pinning techniques are usually recommended for humeral fractures because these fractures are commonly displaced. Correct placement of an intramedullary pin is essential to avoid damage to intra-articular structures during pin insertion.39 Techniques for normograde and retrograde insertion of intramedullary pins into the humerus have been described.8,39,44,87 A study evaluating articular damage from intramedullary pins inserted into the humerus in a directed retrograde, nondirected retrograde, or normograde fashion revealed that 20% of pins passed in a nondirected retrograde fashion penetrated the shoulder joint. The results of this study suggest that although nondirected retrograde pinning cannot be recommended, normograde or retrograde pins directed craniolaterally provide acceptable techniques for insertion of intramedullary pins during distal humeral fracture repair in dogs.82 For proximal normograde insertion, the pin is usually started from the craniolateral aspect of the greater tubercle. For fractures involving the mid- or proximal diaphysis, the pin is driven distally to a point just proximal to the supratrochlear foramen. For fractures involving the distal third of the diaphysis, a pin of smaller diameter is used. The pin should be directed toward the medial side of the shaft, so the tip bypasses the supratrochlear foramen and is embedded in the medial epicondylar crest18; once the pin has entered the distal bone fragment, the bone fragments should be bowed slightly medially to help direct the tip of the pin down into the medial aspect of the condyle. The pin is then cut short at the entry point near the greater tubercle or is left long to be bent laterally and tied-in to an external skeletal fixator. Alternatively, a distal normograde technique can be used, whereby a small pin can be started from the medial aspect of the condyle, placed directly across the reduced fracture, and advanced into the greater tubercle. Once the pin penetrates the greater tubercle, the distal point is cut short, the pin chuck or drill is applied to the pin exiting at the greater tubercle, and the distal point of the pin is drawn into the trochlea, with the proximal pin end then cut as short as possible.41 The distal normograde technique is often used for supracondylar or distal humeral fractures. For retrograde insertion, the pin is placed into the proximal segment from the fracture site and is directed craniolaterally to exit at the greater tubercle. The pin then is partially withdrawn and is advanced distally once the fracture is reduced in a similar manner as for the proximal normograde insertion previously described. For distal fractures, the pin can also be inserted via a distal retrograde technique. The pin is started from the distal fracture site and is passed into the medial epicondylar crest and out of the bone distally. The fracture is then reduced, and the pin passed proximally into the humeral diaphysis. This method allows assessment of the diameter of the medial epicondylar crest for more accurate implant selection. The tapering shape of the humerus does not readily lend itself to interlocking nail fixation in the dog and cat. Fractures often affect the distal aspect of the bone,5 so there is often only room for placement of one locking device (screw or bolt—see Chapter 43) to lock the nail in the distal segment,20 and this may not provide sufficient implant stability. Additionally, the quality and thickness of the cortex in the most proximal aspect of the bone do not enhance screw holding power. Despite anatomic constraints, the use of interlocking nails for stabilization of both canine and feline humeral fractures has been described.20,21,61 Technically, it is often easier to place an interlocking nail into the medullary canal of a bone than to contour a plate to conform to the curvature of the bone surface, especially when fractures of the humerus are treated.20 Suitable fractures for interlocking nail fixation are mid-diaphyseal, with sufficient bone on each side of the fracture to allow placement of two locking devices to lock the nail proximal and distal to the fracture, with locking devices placed at least 1 bone diameter away from the fracture line (Figure 52-6, A). Complications identified with interlocking nail repair of humeral fractures include fracture collapse, osteomyelitis, the screw missing the nail hole, and radial neuropraxia.20,61 Fracture collapse can occur when a bone segment is stabilized with a single screw. If only a single screw is used in the proximal segment, it should be placed distal to the tricipital line, where the bone quality is better, providing improved holding power and therefore less chance that the screw or bolt will loosen and pull out.61 A single screw may not provide sufficient stability, except in very young dogs. The relatively large size of the interlocking nail inhibits placement through the medial epicondylar crest,69 although recommendations have been made to direct the nail into the medial aspect of the humeral condyle, taking care that it does not penetrate the olecranon fossa.20 The proximal end of the nail should not be allowed to protrude from the greater tubercle; otherwise it may cause soft tissue irritation.20 External skeletal fixators have been used successfully for humeral fracture stabilization in both dogs and cats.7,31,45,47 Unilateral type I, modified type I/II (with a full pin across the condyle), or external skeletal fixator frames tied into the intramedullary pin can be used. When used in combination with an intramedullary pin to treat simple humeral fractures, a unilateral external skeletal fixator will prevent rotation, shear, and axial compression. With comminuted fracture repair, particularly where bone stock for implant placement is limited proximal and distal to the fracture, external skeletal fixation is used to help prevent shear, bending, compression, and torsion. Use of an external skeletal fixator may minimize interference with the blood supply, if dissection and manipulation of fracture fragments are limited during application. The humerus does not have a safe corridor for pin insertion; therefore hazardous corridors are identified as the safest areas.56 Increased morbidity is associated with external skeletal fixators applied to the humerus when compared with those applied distal to the elbow joint because of increased muscle mass and soft tissue movement around the elbow, although cats and smaller dogs seem to suffer less morbidity than larger dogs. For simple fractures or fractures with a small amount of comminution, particularly in larger patients, internal fixation may be a preferable option to external skeletal fixation. External skeletal fixation of highly comminuted fractures, particularly fractures of the supracondylar area in which stabilization with internal fixation is challenging, may allow a better biologic approach.4,31,45,47 The objective with external skeletal fixator application is to attain spatial alignment of the two main segments and positioning of the fixation device with minimal disruption of soft tissues (Figure 52-7).
Fractures of the Humerus

Anatomy
Fractures of the Humerus in the Dog and Cat
FRACTURE LOCATION
DOG (%)
CAT* (%)
Proximal
5
2
Diaphyseal
42
75
Supracondylar
15
18
Condylar
44
5
Proximal Humeral Fractures
Proximal Physeal Fractures
Proximal Metaphyseal Fractures
Diaphyseal Fractures
Surgical Approach
Fixation Methods
Conservative Treatment or External Coaptation for Humeral Fractures
Intramedullary Pinning for Humeral Fractures
Interlocking Nailing for Humeral Fractures
External Skeletal Fixation for Humeral Fractures
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Fractures of the Humerus

Only gold members can continue reading. Log In or Register to continue
