Chapter 14 Fecal Incontinence
Definition
Fecal incontinence is defined as the inability to retain feces in the colon and rectum leading to uncontrolled leakage of fecal material at times other than during conscious defecation. The recorded prevalence of fecal incontinence is 43 of 260,000 admissions to the University of Missouri and University of California Veterinary Medical Teaching Hospitals.1 This is probably an underestimation of the true incidence of the disease. There is no sex predilection, but the majority of affected animals are 11 years of age or older. Although fecal incontinence in itself is not a significant cause of morbidity in cats and dogs, it can be a clinical sign associated with serious disease. It can be disastrous for a household pet irrespective of the underlying cause because it commonly leads to euthanasia.
Pathophysiology and Mechanisms
Storage Phase
During formation and storage of feces, distal colonic longitudinal contractions are inhibited by sympathetic activity. The main sympathetic supply to the distal colon and anorectum originates at L2-L5, synapses in mesenteric ganglia, and exits within the hypogastric nerve. Sympathetic stimuli via hypogastric and lumbar colonic nerves inhibit defecation in part by inhibiting colonic contractions. The site of inhibition appears to be in the caudal mesenteric and pelvic plexuses through synapses on parasympathetic motor neurons within vagal and pelvic nerves, respectively. The pelvic plexus lies lateral to the middle portion of the rectum.2
Fibers from lumbar colonic and hypogastric nerves also innervate the IAS leading to contraction.3 Thus the internal anal sphincter is important in maintaining the resting pressure of the anal canal.4,5 The region of increased tone extends from approximately the pelvic brim to the anus. Coordination of colonic contraction and sphincter relaxation occurs in the enteric nervous system, notably the pelvic plexus. Injury to the autonomic nerve fibers in the pelvic plexus may lead to fecal incontinence after resection of part of the distal colon or rectum. However, resection of the IAS does not necessarily completely interfere with fecal continence.4
Awareness of the Need to Defecate
As feces form in the descending colon, occasional peristaltic waves push material distally into the rectum. In dogs, feces arriving from the colon are halted at the rectocolonic junction by sphincteric pressure, thus stool stops short of the rectocolonic junction instead of passing directly to the rectum.6 Rectal tone is maintained mostly through sympathetic innervation.7 Expansion of the rectal walls stimulates stretch receptors that send afferent signals through the pelvic nerve to ascending spinal cord tracts that ultimately lead to the frontal cortex. This leads to the awareness of the urge to defecate. Afferent fibers in the pudendal nerve convey the sensation to reinforce urge when fecal material extends to the level of the anus. A reflex arc is present whereby even slight distention of the rectum of humans or dogs results in relaxation of the IAS. This is the rectosphincteric inhibition reflex.8 This arc is suppressed by upper motor neurons (UMNs) until the conscious decision is made to initiate defecation. Thus a disturbance of descending UMNs decreases inhibition. Contraction of the IAS is unlikely to be important in maintaining continence when pressure in the rectum becomes high, but may help guard against incontinence of small amounts of liquid stool. Additionally, reflex relaxation of the IAS in response to rectal distention allows for conscious “sampling” of the rectal contents and helps distinguish flatus from feces.
Defecation Phase
At the appropriate time, the impulse for defecation originates in the cerebral cortex and descends via motor tracts through the brainstem to the lower motor neurons of sacral, pelvic, and pudendal nerves leading to relaxation of the IAS. During normal defecation, there is relaxation of the rectum prior to colonic contraction, then migrating contractions of the colon pass aborally to the rectum. The IAS muscles continue to relax while large amplitude contractions of the colon migrate to the rectum.4,9
Migrating colonic contractions under control of the pelvic and sacral nerves advance fecal material into the rectum. The rectum shortens as material is forced into the anal canal and peristaltic waves propel feces out of the rectum. Relaxation of the IAS is achieved by inhibitory reflexes carried predominantly by pelvic and sacral nerves to the mesenteric plexuses.10 This inhibitory reflex is absent in animals with a congenital absence of distal colonic ganglionic neurons (Hirschsprung disease) causing failure to relax and functional colonic obstruction.11 Vagal nerve function may compensate for denervation of the pelvic nerve leading to recovery of defecation reflexes after several weeks 12 Finally, somatic inhibition of skeletal muscle of the EAS via the pudendal nerve permits defecation into the animal’s environment.
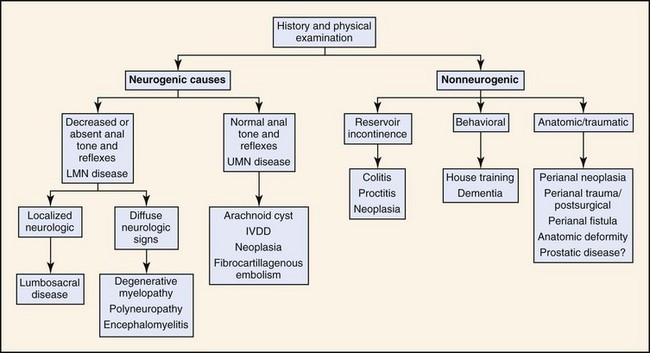
Overall coordination of defecation involves parasympathetic nervous system (via the vagus and pelvic nerves), sympathetic nervous system (via the hypogastric nerve), and somatic nervous system (via the pudendal nerve). Fecal incontinence can occur because of failure of storage (reservoir incontinence), failure of UMN control (UMN incontinence), or failure of IAS and EAS contraction (sphincter incontinence). Box 14-1 and Figure 14-1 outline causes of fecal incontinence.
Box 14-1
Causes of Fecal Incontinence
Sphincter Incontinence
Failure of tonic anorectal and anal sphincter tone can occur due to trauma to the pudendal nerve, as part of cauda equina syndrome, or as part of more generalized degenerative or inflammatory neuropathies such as degenerative myelopathy of German Shepherds. Neurogenic sphincter incontinence is most commonly associated with lower motor neuron dysfunction, as seen with lumbosacral disease. Animals with lumbosacral disease often have decreased anal tone, decreased anal and rectal sensation, and loss of the rectosphincteric reflex. In a study of 69 surgically treated cases of degenerative lumbosacral stenosis in dogs, four (6%) had fecal incontinence prior to surgery, and of those only one improved without surgical correction.13 Following dorsal decompressive laminectomy, a further four developed fecal incontinence. Although rare in cats, lumbosacral disease is occasionally seen and has been associated with fecal incontinence.14 Perianal surgical procedures can result in damage to the EAS or its innervations leading to incontinence.15–17
Aging has a gradual and progressive effect on anal function. Effects of aging in human colon and anal sphincter include thinning of the external anal sphincter, weakening of muscular contraction, and increased latency of pudendal nerve firing.18 This may be relevant to geriatric dogs and cats.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


