Chapter 13 Dysphagia and Gagging
Definition
The term dysphagia derives from the Greek roots dys, meaning “difficulty” or “disorder,” and phagia, meaning “in eating.” Broadly defined, dysphagia would apply to a large number of oropharyngeal disorders for which there is difficulty in eating. Thus the term could be used to describe problems associated with prehension of food or water, bolus formation, rostral-to-caudal contraction of pharyngeal constrictor musculature, dropping of food and/or water from the commissures of the mouth, and swallowing. Over time, dysphagia has become more strictly defined as difficulty in swallowing. Gagging or the gag reflex is an involuntary retching reflex stimulated by mechanical irritation of the posterior palate or pharynx. Dysphagia may provoke gagging, but gagging does not necessarily imply dysphagia. Regurgitation is a clinical sign more consistent with esophageal disease and should be differentiated from dysphagia, gagging, and vomiting (see Chapter 21). Regurgitation differs from vomiting in that it is characterized by passive retrograde evacuation of undigested food from the esophagus. Vomiting is characterized by coordinated activities of the gastrointestinal, musculoskeletal, and nervous systems culminating in the active evacuation of digested or partially digested food from the gastrointestinal tract (see Chapter 23).1 Vomiting usually signifies disease caudal to the gastroesophageal sphincter. Signs referable to aspiration pneumonia, for example, coughing and dyspnea, may be the major presenting complaint in some animals. A good history will usually differentiate these signs from others (e.g., dysphagia, gagging) associated with oropharyngeal disorders.
Pathophysiology and Mechanisms
The oropharyngeal phase of swallowing is subdivided into three stages.2–6 The first or oral stage begins with prehension of food with teeth and tongue and formation of the bolus at the base of the tongue. In the second or pharyngeal stage, rostral to caudal pharyngeal contractions propel the bolus from the base of the tongue to the cricopharyngeal or cranial esophageal sphincter opening. Mechanical stimulation of the caudal pharynx activates an afferent neural pathway that has its synapse in the brainstem, and which activates an efferent neural pathway back to the cricopharyngeus leading to inhibition and relaxation. The cricopharyngeus relaxes during the third or cricopharyngeal stage, and the bolus passes into the cranial esophageal body (Fig. 13-1). The cricopharyngeus subsequently contracts, pharyngeal muscles relax, and the oropharyngeal phase is repeated with successive swallows.
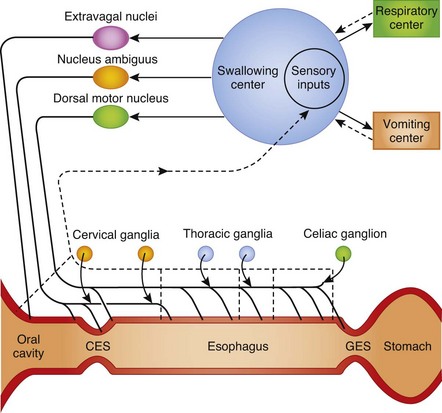
Figure 13-1 Neural regulation of swallowing in the dog and cat.
(Reprinted with permission from Washabau RJ, Holt DE. Pathophysiology of gastrointestinal disease. In: Slatter D, ed. Textbook of small animal surgery, 3rd ed. Philadelphia, Saunders, 2003.)
Abnormalities in any of the oropharyngeal stages can produce oropharyngeal dysphagia.6 Oropharyngeal dysphagias are either morphologic or functional in origin. Morphologic disorders that interfere with oropharyngeal phase of swallowing include strictures, foreign bodies, and neoplastic, traumatic, and inflammatory processes of the oral cavity and pharynx. Most functional disorders consist of failure, spasticity, or incoordination of muscular contractions and are due to neuromuscular diseases.
Differential Diagnosis
Oropharyngeal Dysphagia
Three types of oropharyngeal dysphagia have been characterized in companion animal species: (a) oral stage dysphagias with prehension deficits mainly as a consequence of loss of tongue function; (b) pharyngeal stage dysphagias with transport deficits mainly as a consequence of loss of cranial and caudal pharyngeal constrictor function; and (c) cricopharyngeal stage dysphagias with cricopharyngeal opening or closure (achalasia or chalasia) deficits, or incoordination between pharyngeal contraction and cricopharyngeal sphincter relaxation.6,7 Neuromuscular disease is the underlying pathogenesis of oropharyngeal dysphagia, but precise etiologies are rarely identified. Some cases have been associated with brainstem disease, peripheral neuropathy, myasthenia gravis, polymyositis, muscular dystrophy, and hypothyroidism. A unique form of oropharyngeal dysphagia bearing some resemblance to muscular dystrophy has been described in the Bouviers des Flandres breed (Table 13-1) 8,9
Table 13-1 Known Breed Predispositions for Diseases of the Oropharynx Causing Dysphagia and Gagging
| Condition | Breed |
|---|---|
| Oral neoplasia | Golden retriever, Weimaraner, Boxer, Cocker Spaniel |
| Oropharyngeal dysphagia | Bouvier des Flandres, Golden Retriever, Labrador Retriever |
| Oral eosinophilic granuloma | Siberian Husky |
Evaluation of the Patient
History
Dysphagia and gagging are the most important clinical signs with oropharyngeal disorders. Pet owners may also describe difficulties in drinking water or forming a solid bolus, excessive mandibular or head motion, persistent forceful ineffective swallowing efforts, dropping of food from the mouth, nasal discharge because of misdirection of food into the nasopharynx, excessive salivation, foaming from the mouth, coughing, failure to thrive, and reluctance to eat.6,10 Regurgitation, a common sign of esophageal disease, is less frequently reported with oropharyngeal dysphagias.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


