57 Episcleritis
CLINICAL EXAMINATION
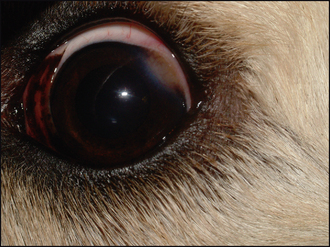
General clinical examination is unremarkable. On ophthalmic examination the most obvious abnormality is the red eye. Marked episcleral congestion will be present, together with some overlying conjunctival hyperaemia. Thus the superficial conjunctival vessels – the thin bright red branching ones – will be engorged, while the deeper, darker, straighter episcleral vessels will be thickened and more tortuous than usual. There will be some diffuse swelling in the area but this will not be excessive (not true chemosis) (Figure 57.1).