Kate Allen, Samantha H. Franklin
Dynamic Endoscopy
It is now acknowledged that endoscopy of the exercising horse is required for definitive diagnosis of dynamic upper respiratory tract (URT) collapse. Although endoscopy of the resting horse is useful for identifying static obstructions and is a reasonably sensitive method for prediction of arytenoid cartilage abduction during exercise, many studies have shown endoscopy at rest to be unreliable for diagnosis of other dynamic conditions affecting the URT.
Since the late 1980s, dynamic upper respiratory tract endoscopy has been possible during exercise on a high-speed treadmill. This technique has led to the diagnosis of a wide spectrum of dynamic obstructive conditions affecting the larynx and nasopharynx. However, the number of horses examined in this manner was small relative to the number of horses in which URT surgery was performed without a definitive diagnosis. There was a clear need for a low-cost field-based technique that would enable definitive diagnosis of dynamic disorders to be made before surgery. Initial research focused on analysis of respiratory sound recordings, but it became apparent that this technique also had diagnostic limitations because many URT obstructions produce sound waves in the same frequency range. Therefore an endoscopic system was required, and this led to the development of portable telemetric systems (overground endoscopy). Endoscopic examination of the URT during field exercise has a number of advantages over use of a high-speed treadmill. The exercise test can be conducted in the environment typically used for competition, and horses may be examined in a manner appropriate to their discipline. In addition, the effects of the tack and rider are accounted for.
The first clinical trial in 2008 confirmed the feasibility of overground endoscopy and proved that diagnostic images of the URT could be obtained during ridden exercise. Subsequent publications by different authors, using various dynamic endoscopy systems, have confirmed the value of this new technique.
Equipment
Several overground endoscopy systems are available commercially, but because the technology is in its early stages of development, systems are likely to improve over the forthcoming years. In most cases the systems are comprised of an insertion tube attached to a telemetric unit that is fitted directly onto the horse. The endoscopy image is transmitted to a hand-held screen for the veterinary surgeon to view in real time. Some systems are mounted on the horse’s head, whereas others have the processor, telemetric unit, and battery pack mounted on the saddle pad or in a backpack carried by the rider (Figures 51-1 to 51-3). Initially there were concerns about rider safety with the rider-mounted systems; however, some clinicians have used these systems extensively, and thus far no incidents have been reported. Miniaturization is still an issue with several systems. At present. improved miniaturization tends to come at the cost of light output, steering of the endoscope tip, and inclusion of an air-water pump. Transmission distance varies with the units, but usually depends on a direct line of sight over distances of 100 to 200 meters. Units with remotely operated air-water pumps are preferred because obscuring of the image by mucus on the camera lens is a common problem. When automatic flush is unavailable, the horse has to be stopped, the endoscope cleaned and replaced, and then exercise restarted. Ideally it should be possible for air and water to be selected on demand. However, some systems only have the capacity to set the water to flush at predetermined intervals, which can result in unnecessary volumes of water within the nasopharynx, and this can stimulate excessive swallowing during exercise. The endoscopy images are recorded onto a hard disk, and it is important to be able to play back the images in slow motion and frame by frame to allow comprehensive review.


Typically the equipment is placed on the horse while it is still in the stable. The horse then undertakes a short warm-up to become accustomed to the equipment before the actual exercise test is performed. It is not uncommon for head shaking or snorting to occur while the horse is at rest or walking, but this almost always ceases as soon as faster exercise begins. Many clinicians evaluating racehorses also use a GPS monitor, with or without heart rate monitor or electrocardiogram, to objectively assess speed, distance, incline, and exercise intensity during the diagnostic evaluation.
Exercise Testing
The type of exercise test performed is crucial for establishing a definitive diagnosis of dynamic airway collapse and will differ for racehorses and other sports horses.
Sport Horses
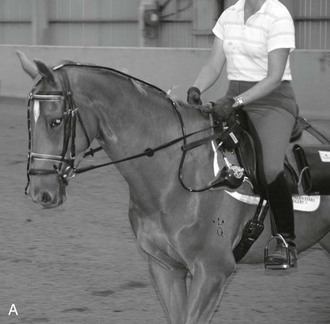
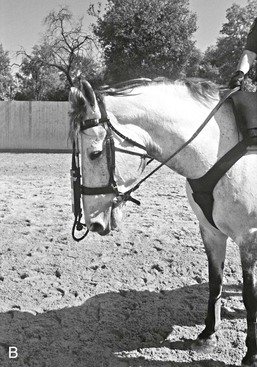
Overground endoscopy appears to be an effective technique for assessment of dynamic upper respiratory tract collapse in sport horses. In these horses, head and neck flexion is often influential in exacerbating the URT collapse. Head and neck flexion affect upper airway flow mechanics during exercise and is thought to play a role in several forms of URT collapse. Dressage horses and show jumpers are typically examined in an arena and are asked to perform a similar level of exercise in an appropriate degree of head and neck flexion for that specialty. During overground endoscopy, the rider can repeatedly change between extended and flexed head positions to observe the effect on the URT. For event horses, dynamic URT obstruction most commonly occurs during the cross-country phase, so exercise on the gallops should be undertaken to recreate the problem during fast work.
In a comparison of the results of overground endoscopy and treadmill endoscopy in nine sport and leisure horses, three horses developed more obvious or different URT obstructions only under ridden exercise and not during treadmill exercise. It is probable that this results from the greater head and neck flexion imposed during ridden exercise than during treadmill exercise. A more recent study reported the diagnostic findings in 129 sport horses undergoing overground endoscopy, 106 of which had a diagnosis of some form of URT obstruction. Both head and neck flexion and rider intervention resulted in exacerbation of URT obstruction in 90% of the horses. The effect of rider interventions such as tightening of the reins, application of spurs, abrupt transitions between gaits, and working in tight circles or sudden changes in direction resulted in exacerbation of URT collapse in 81% of cases. Both situations had a more significant effect on the development of URT obstructions in dressage horses than in show jumpers, possibly because dressage horses are usually ridden with a greater degree of head and neck flexion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


