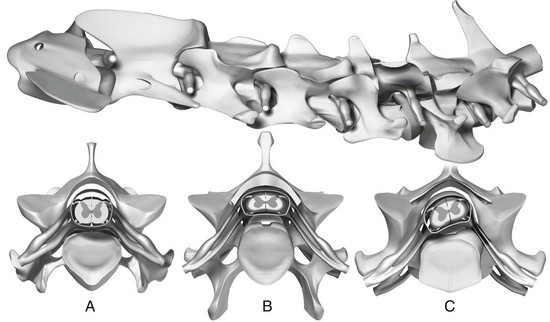
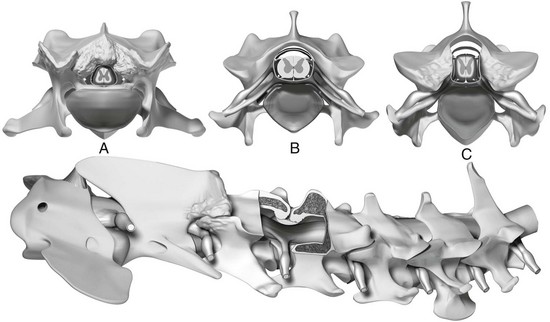
Chapter 236 Disk-associated compression typically is seen in middle-aged large-breed dogs (mostly Dobermans). It is caused by intervertebral protrusion with or without hypertrophy of the dorsal longitudinal ligament or ligamentum flavum (Figure 236-1). Three factors act in combination to explain the pathophysiology of disk-associated CSM: (1) relative vertebral canal stenosis, (2) more pronounced torsion in the caudal cervical spine leading to intervertebral disk degeneration, and (3) protrusion of larger-volume disks into the caudal cervical spine. Affected dogs apparently are born with a congenital vertebral canal stenosis that predisposes them to the development of clinical signs. Figure 236-1 Disk-associated cervical spondylomyelopathy. Top: Ventral spinal cord compression and nerve root compression at C5-6 caused by intervertebral disk protrusion. Dorsally, hypertrophy of the ligamentum flavum causes mild spinal cord compression. A, Transverse section at the level of the C4-5 disk region showing normal spinal cord and vertebral canal. B, Ventral compression at the C5-6 region caused by intervertebral disk protrusion and hypertrophy of the dorsal longitudinal ligament and ligamentum flavum (leading to mild dorsal compression). C, Asymmetric intervertebral disk protrusion at C6-7 causing spinal cord and nerve root compression. The vast majority of disk-associated spinal cord compressions are located in the caudal cervical spine, affecting the disks at C5-6 and C6-7. The biomechanical features of the caudal cervical spine explain the high incidence of lesions there. This region experiences three times more axial rotation or torsion than the cranial cervical spine, and torsion (more than axial compression) is the main biomechanical force leading to intervertebral disk degeneration in nonchondrodystrophic dogs. Additionally, a study found that Dobermans with CSM have larger intervertebral disks than clinically normal Dobermans (da Costa et al, 2006b). This would cause a larger volume of disk protrusion into the vertebral canal. Since dogs with CSM have a narrow vertebral canal, the combination of a stenotic vertebral canal and protrusion of disks with larger volumes ultimately leads to clinical disease. The pathophysiology of osseous or bony CSM is different. Osseous CSM is seen predominantly in young adult giant-breed dogs, especially in Great Danes. Although a hereditary basis still is unproven, a familial predisposition has been identified. Giant breeds usually have severe absolute vertebral canal stenosis secondary to proliferation of the vertebral arch (dorsally), articular facets (dorsolaterally), or articular facets and pedicles (laterally) (Figure 236-2). The cause of the compression appears to be a combination of vertebral malformation and osteoarthritic-osteoarthrotic changes at the level of the articular facets. Even though most giant-breed dogs have osseous compression, occasionally these compressions are complicated by disk protrusion, especially in older dogs. Ligamentous compression (by the ligamentum flavum) may be involved in the pathophysiology of the disease in giant- and large-breed dogs, but pure ligamentous compression as the single source of compression appears uncommon. Figure 236-2 Osseous cervical spondylomyelopathy. A, Severe dorsolateral spinal cord compression at C2-3 caused by osseous malformation and osteoarthritic changes. B, Normal C3-4 disk region. C, Bilateral compression at C4-5 caused by osteoarthritic changes and medial proliferation of the facets resulting in absolute vertebral canal stenosis and foraminal stenosis, which lead to spinal cord and nerve root compression, respectively. Bottom: Dorsal spinal cord compression at C3-4 caused by lamina malformation and hypertrophy of the ligamentum flavum. Osteoarthritic changes also are shown at C2-3. The most common location of compressive lesions in both large- and giant-breed dogs is at C5-6 and C6-7. The lesion is located at one of these sites in 90% of affected large-breed dogs. In giant-breed dogs, the C4-5 site also is commonly affected. Approximately 50% of large-breed dogs have a single site of spinal cord compression, and 50% have two or more sites of similar severity. In giant-breed dogs approximately 20% of dogs have a single site of compression, whereas 80% have multiple compressive lesions. A computed tomographic (CT)–myelographic study identified lesions affecting the T1-T2 and T2 regions in 14% of giant-breed dogs and the C7-T1 region in 22% of all dogs (da Costa et al, 2012). These lesions were not the primary site of compression but were part of the multiple compressions seen in giant-breed dogs. For this reason, it is important to include the cranial thoracic region in imaging studies of dogs suspected of having CSM.
Diagnosis and Treatment of Cervical Spondylomyelopathy
Causes and Pathophysiology
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


