16 Complicated keratoconjunctivitis sicca
CLINICAL EXAMINATION
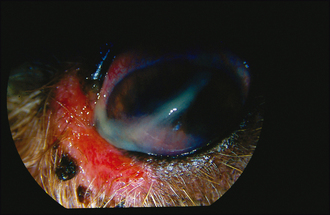
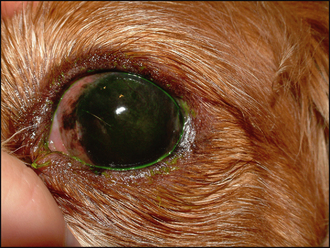
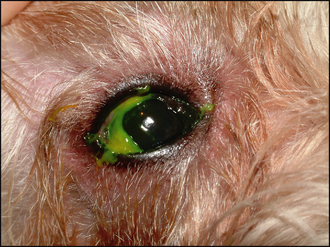
Unless the dog has a systemic disease which can exacerbate KCS, such as diabetes mellitus, hypothyroidism or hyperadrenocorticism, general clinical examination is usually unremarkable. On initial ophthalmic assessment the most striking problem is the copious mucopurulent discharge. A sample should be taken for culture and sensitivity before gently wiping this away. Conjunctival hyperaemia and hyperplasia will be apparent. Schirmer tear test readings are expected to be bilaterally low – probably less than 2 mm of wetting in a minute. The periorbital skin might be inflamed and thickened, or even slightly ulcerated if a chronic blepharitis has been present or the patient has self-traumatized (Figure 16.1). The cornea is likely to be pigmented either across the dorsal half or sometimes covering most of its surface (Figure 16.2). Many dogs can still see and retain a menace response despite significant pigmentary keratitis. Branching superficial blood vessels will also be present, and sometimes a slight granulation tissue reaction is also noted, particularly if previous ulceration has occurred. In poorly responsive or neglected cases of chronic KCS ulceration is not always a feature. Once the discharge is cleared away corneal examination will show a dull, lacklustre surface with some epithelial irregularity but not true ulceration. Careful irrigation of excess fluorescein dye is required to prevent false positives as the dye pools in the irregular surface or sticks to the mucus (Figure 16.3).
Acute ulceration associated with KCS is typically deep and central (Figure 16.4). Thus a facet is clearly visible in the central or subcentral cornea and surrounding corneal oedema can be present. If the secondary bacterial infection is severe then keratomalacia might be present such that the ‘melting’ cornea around the ulcer has a gelatinous appearance. Fluorescein staining will be positive, but it is not uncommon for a descemetocoele to be present such that only the sides of the ulcer retain dye with the central area remaining dark, representing Descemet’s membrane. Some peripheral corneal pigmentation and superficial vascularization might also be noted, reflecting the chronicity of the underlying KCS. A reflex uveitis and miotic pupil might also be noted.

The definitive diagnosis of keratoconjunctivitis sicca has already been made. However, other exacerbating factors such as entropion, lagophthalmos, blepharitis and systemic disease might be present and should be considered. A list of the possible causes of KCS is provided in Table 16.1.
Table 16.1 Possible causes for keratoconjunctivitis sicca (KCS)
| Possible causes for KCS | Comment |
|---|---|
| Immune-mediated lacrimal gland disease (most common) | Most common |
| Congenital lacrimal gland aplasia | E.g. Cavalier King Charles spaniels, Jack Russell terriers |
| Drug suppression of lacrimal gland | E.g. atropine drops |
| Drug toxicity and damage to lacrimal gland | E.g. sulfasalazine and sulphonamides |
| Lacrimal gland adenitis | Distemper virus and some cases of conjunctivitis and blepharitis will have lower Schirmer tear test readings |
| Traumatic injury to lacrimal gland | Road traffic accident with head trauma |
| Neurogenic | Lack of parasympathetic supply to lacrimal glands |
| Other neurological signs sometimes present | |
| Prior removal of nictitans gland | Prolapsed nictitans glands are more common in the same breeds that are predisposed to KCS and gland removal is not recommended |
| Systemic disease | Hypothyroidism, hyperadrenocorticism, diabetes mellitus |
EPIDEMIOLOGY
There are several causes for KCS in dogs (see Table 16.1) and its incidence is reported at about 1% of the population of dogs presented to North American Veterinary Colleges. Certainly a breed predisposition is noted with immune-mediated KCS, so a presumed inherited component is present, although details of this have not been elucidated, and many other factors are clearly involved. English bulldogs, West Highland white terriers, Cavalier King Charles spaniels, American and English cocker spaniels and pugs are among the many breeds commonly seen with the condition. A sex predisposition to females has been reported in West Highland white terriers.



