5 Complicated entropion
CLINICAL EXAMINATION
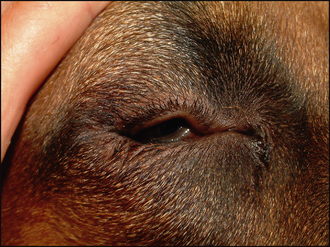
Menace responses should be normal providing the dog is able to open its eyes sufficiently to be assessed! However, they might trigger an intense blepharospasm such that further examination is difficult. Providing there is no evidence of keratoconjunctivitis sicca (in which case a Schirmer tear test should be performed first), a drop of topical anaesthetic can be applied to the cornea to relieve the trigeminal pain and ease further examination. This will also remove any spastic component to the entropion such that the degree of anatomical entropion can be assessed. The lid margin will typically be wet, and is often slightly depigmented along the area of inversion (Figures 5.1 and 5.2). It can be gently rolled out but will immediately start to roll inwards again. Many dogs will have elevation of their nictitans membranes and possibly some degree of enophthalmos as a result of chronic corneal pain and this should also be reduced following the application of topical anaesthesia. Conjunctival hyperaemia will be present and varying degrees of corneal damage will be noted. This can range from very slight irregularity of the corneal epithelium, fine superficial vascularization, overt ulceration of differing depths and scarring and granulation tissue. In very severe cases of entropion, particularly in young Shar Pei puppies, the rubbing from the eyelid hair can have been so severe as to cause almost total corneal granulation or sometimes corneal rupture (see Case example 5.1).

In addition to assessing the position of the eyelids it is important to consider the canthi, especially in large breed dogs. Normally the medial and the lateral canthus should be in the same horizontal plane, but with laxity at the lateral canthus – for example, in giant breeds with ‘diamond eye’ – this can slip ventrally giving a sloping appearance to the palpebral fissure (Figure 5.3). The skin at the lateral canthus can be rolled in (lateral canthal involution) which is common in breeds with large skulls such as Rottweilers and retrievers, especially male dogs, and is due to a tight and abnormally positioned lateral canthal ligament. This sometimes needs addressing along with the entropion, discussed in the case below (see Case example 5.2).

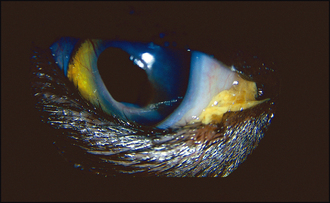
Other ocular abnormalities such as distichia might accompany the entropion and it is essential to determine whether they are significant in the pathogenesis. Similarly, if a corneal ulcer is present this might have been the primary problem, with entropion developing secondary to the trigeminal pain. Secondary entropion can follow from corneal sequestrum formation in cats (Figure 5.4). A mild reflex uveitis might be noted on intraocular examination but often the rest of the examination is unremarkable.
EPIDEMIOLOGY
TREATMENT OPTIONS – SURGICAL
For uncomplicated cases of entropion a simple Hotz-Celsus procedure under general anaesthesia, removing an ellipse of skin parallel to the in-turning, is very successful. The steps for how to do this are detailed in Table 5.1. However, we will concentrate on the more complicated cases – and only the more commonly encountered types of these. Some very complex lid abnormalities, such as diamond eye with lateral canthal laxity, might be better referred to an experienced ophthalmic surgeon.
Table 5.1 Steps for performing a Hotz-Celsus procedure
| Procedure | Effect | |
|---|---|---|
| 1 | Decide on area of skin requiring excision prior to sedation but after the application of topical anaesthetic | Removes the spastic component of the entropion leaving purely the anatomical abnormality |
| 2 | Perform initial skin incision parallel to lid margin, 1–2 mm away | Close as possible to lid margin for most everting effect but sufficient space to place sutures |
| 3 | Incision depth to include orbicularis oculi | Sufficiently deep to have effect |
| 4 | Second incision shaped to provide exact out-rolling of abnormal lid margin | Two incisions meet at gentle point, not abruptly |
| 5 | Excise skin between two incisions | Use rat-toothed forceps and fine scissors such as tenotomy scissors |
| 6 | Suture carefully with 6/0 material in simple interrupted pattern | Place first suture centrally and work out to prevent uneven placement |
| 7 | Ensure knots are away from lid margin and cut suture ends short | Ensure nothing can rub to irritate the cornea |
Rottweiler type (Case example 5.1)
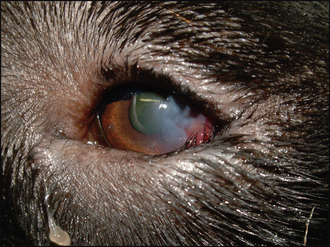
Entropion in large-headed breeds, such as the Rottweiler, can be challenging to treat – although on initial examination it might appear as a straightforward lower lid entropion. Unfortunately, this breed, and others with similar anatomy, frequently develops very intense blepharospasm resulting in corneal ulceration in the ventrolateral quadrant (Figure 5.5). This can develop prior to your intervention, or sometimes a few days following a simple Hotz-Celsus surgery. It is not uncommon for the patient to look fine on a 2-day post-surgery check-up, only to return 48 hours later with a very sore eye with ulceration, marked blepharospasm and further entropion – even with the sutures from the initial surgery now rubbing and exacerbating things. Obviously owners are never happy if this situation develops!
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


