Chapter 18
Chemical immobilization of wild animals
Sonia M. Hernandez
Introduction and general concepts
Prior to capture and anaesthesia
Handling and treatment of accidental exposure to carfentanil or etorphine
Introduction and general concepts
The nature of wild animals dictates that any manipulation that requires handling will necessitate chemical immobilization. Anaesthetizing wild animals is typically done to mark an animal, to apply a radio transmitter, administer individual animal treatment, or for the purpose of research. Anaesthesia of wildlife can be challenging and requires that veterinarians adjust the general principles of anaesthesia to the unique anatomy and physiology of wildlife species and challenging field conditions. Specific anatomical and physiological details are not always available, although the reader is directed to excellent resources for specifics (Fowler & Cubas, 2001; Fowler & Miller, 2003). In most cases, anaesthetic protocols have been adjusted from doses in domestic species and rarely are detailed pharmacokinetic studies available. Unlike working with small animal patients, veterinarians planning to anaesthetize wildlife are not often afforded the opportunity to physically examine patients, or acquire biological samples to assess their physical status prior to anaesthesia, and that sometimes translates to choosing anaesthetic cocktails with a wider safety margin while sacrificing other parameters such as recovery time. Additionally, capture and chemical immobilization of wildlife can pose some significant human safety considerations. Lastly, morbidity and mortality of patients undergoing field anaesthetic procedures is not uncommon. For example, high ambient temperature can lead to hyperthermia.
This review will focus on the general principles of wildlife anaesthesia, with an emphasis on free-ranging North American species; however, for more in-depth information, particularly species-specific details, the reader is directed to more detailed references (Kreeger & Arnemo, 2002; Carpenter, 2005; West et al., 2007). Other texts such as Research and Management Techniques For Wildlife and Habitats are also very helpful for capture, identification and handling of wildlife species (Brookhout, 1996). Veterinarians working with wildlife will benefit from collaboration with wildlife biologists and ecologists who can help design capture techniques that minimize stress and provide invaluable knowledge about the animal’s behaviour. When anaesthetizing a species for the first time, it is very useful to contact zoo and wildlife veterinarians who routinely work with these species for their expertise. Important modification to protocols often take time to be published, yet experienced practitioners have a wealth of knowledge.
Prior to capture and anaesthesia
As much as possible, veterinarians working in wildlife capture teams should become familiar with the anatomy, physiology and population dynamics of the species at hand. In some cases, humane and effective methods of physical capture of wildlife species have been described often negating, or at least facilitating, chemical immobilization (Schemnitz, 1999). The team responsible for the anaesthetic event should meet several times in advance to plan and organize the logistical, equipment and personnel needs for the procedures. It is important to assign each person a specific duty, so that at the time of the anaesthetic procedure everyone’s responsibilities are clear. When working with dangerous animals, a specific person trained and equipped with firearms may be needed. In addition, a visit to the site of capture prior to the procedure is paramount to determine environmental factors, such as landscape characteristics that may pose a threat to the personnel or the animals. Field sites can be rocky, muddy, traversed by creeks that pose a drowning hazard, or cliffs. It may be possible to estimate the time of the day that the animal in question may have had the least amount of food, or remove available food resources. Finally, the team should discuss the realistic potential for morbidity and mortality and should agree on what may be considered an ‘acceptable rate’. For example, when working with common and abundant species, it may be acceptable to expect a 10% loss, while when working with endangered species, even the loss of one individual might not be acceptable. These decisions may translate to utilizing more expensive anaesthetic protocols, or designing back-up plans that require more personnel and equipment.
Anaesthetic procedures should be planned at a time of year and time of day when they pose the least hazard to the species. For example, if working with bears, it is important to take into consideration the metabolic changes associated with hibernation and avoid anaesthesia during this period. Ungulates are best anaesthetized in the early spring or fall and during the coolest period of the day to avoid hyperthermia. On the other hand, in temperate zones, hypothermia during winter months is also a major concern. In addition, vehicles required for the anaesthetic procedure (e.g. helicopters, trucks) may not be efficient during rainy, ice or snowy conditions. Some landscape characteristics can pose real dangers. For example, steep, rocky terrain, or nearby water sources may require additional personnel to corral or herd animals away from danger and working in such conditions requires protocols that produce the shortest induction time. The social hierarchy of some animals may be important if individuals are going to be separated from a group, or if, for example, a herd may become ‘protective’ or aggressive towards an animal showing drug effects, or towards the capture team. Predation can occur, particularly during induction and recovery, before or after the anaesthetic team can protect the animals.
Unfortunately, the body weight of the animal often needs to be estimated. This may prove difficult in larger species that cannot be examined up close prior to darting. However, there are several resources which publish the range of body weight expected for common species (Kreeger & Arnemo, 2002; Fowler & Miller, 2003). The gender, life stage and reproductive status are also important details. For example, xylazine is a common ingredient in anaesthetic cocktails utilized to immobilize free-ranging bison, yet it may cause abortion. All of this information should be carefully recorded. Record sheets should be designed ahead of time to collect important data that can facilitate future anaesthetic periods.
Premedication is rarely possible in wildlife species. However, it may be useful to contain animals in large enclosures and remotely administer neuroleptics, particularly to those species prone to anxiety or stress and particularly if transport is planned. Azaperone has been used to facilitate translocations and zuclopenthixol acetate provides up to 4 days of tranquilization in cervids (Read et al., 2000; Woodbury et al., 2001; Read and McCorkell, 2002).
Capture techniques and remote drug delivery
Physical restraint, whenever possible, will facilitate administration of anaesthesia and reduce stress for the animal. This is particularly useful for small mesopredators (e.g. raccoons, coyotes, otters) in which leghold traps, cage traps or squeeze cages allow the anaesthetist to hand inject, or use a pole syringe (Figs 18.1, 18.2). Small rodents can also be trapped in cage traps, transferred to mesh bags and hand-injected (Fig. 18.3). Other animals may be baited to food sources, or attracted to areas with pheromones, allowing the anaesthetist to see and dart them more easily. If physical restraint is not possible, animals may need to be located and chased with the use of hunting dogs, helicopters or trucks (Fig. 18.4).

Figure 18.1 A river otter was transferred directly from its transport cage to a laboratory animal-type squeeze cage where it can easily be hand-injected.

Figure 18.2 A Havahart style cage has been modified with a removable welded-bar piece that allows for the biologist to hand inject a raccoon. Photo courtesy of M. J. Yabsley.

Figure 18.3 A pocket gopher was first trapped in a modified cage trap, then transferred to a zippered mesh bag for hand injection of anaesthetic agents.

Human safety
Chemical immobilization of wildlife is inherently a dangerous job, particularly for those that lack experience (Caulkett & Shury, 2007). It is wise for at least two people in the team to be trained in safety, first aid and CPR. It is also useful, particularly when working with anaesthetics in the field, that a relationship has been established with a nearby hospital or physician who is familiar with field chemical immobilization procedures. Human safety should be paramount in any chemical immobilization procedure and the team leader should not be afraid to cancel or postpone a procedure if human safety is at risk of being compromised. There are a variety of hazards that can be encountered and easily overlooked. As mentioned before, the capture team should become intimately familiar with the terrain, weather conditions and equipment available at the field site well in advance to any procedure to identify potential hazards. Procedures can take longer than expected and the team should be prepared for a variety of situations, including incoming inclement weather.
The team should be composed of someone who is very familiar with the behaviour of the animal to be immobilized. Most animal species have some inherent defence system, particularly when chased, trapped or cornered. Hill et al. (1998) reported on the increase of animal-related injuries to veterinarians working with wildlife. If an animal is cornered, formulating an escape route for the capture team should be discussed in advance. Although the danger associated with some species like carnivores is obvious, ungulates can be just as lethal, especially aggressive males during rut. Even when anaesthetized, premature arousal or stimulation can cause an animal to bite or kick. Large ungulates should be hobbled and other forms of physical restraint, such as a dedicated person holding the head of a carnivore, are wise. Members of a herd can become curious or aggressive towards the capture team (Fig. 18.5).
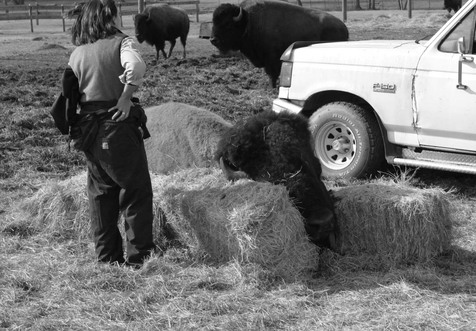
Figure 18.5 An immobilized North American bison in sternal recumbency is surrounded by trucks and personnel to protect the capture team from the rest of the curious herd.
Darts and dart delivery equipment should be treated like firearms. Anyone handling the equipment should be adequately trained. Shooting should not take place in areas where a person may inadvertently become the target. Drug exposure or other types of injury (e.g. inadvertent needle sticks, explosions) usually occur when darts are being loaded. Ideally, a dart should be loaded in a quiet place where the loader is not distracted by the activities of the capture, but where at least another person can watch the loader in the event of injury. The loader should wear minimum standard personal protective equipment, including gloves, long sleeve attire and a face shield. Damaged darts sometimes cannot be identified until they are pressurized and thus the same equipment should be donned when a dart is pressurized. Not uncommonly, in two-chambered gas darts, the needle is not secured properly and can shoot forward when the dart is initially pressurized. The author always uses a large empty syringe case slipped over the dart while it is being pressurized. When working with large dangerous species, a dedicated, trained security person with a backup firearm is essential. This person should be adequately trained and familiar with the firepower necessary to incapacitate the species at hand.
Most anaesthetics pose some safety hazard for people. The ‘super narcotics’ (etorphine and carfentanil) can cause rapid, severe and profound sedation, respiratory depression, hypotension and cardiac arrest. For perspective, carfentanil is 10 000 times as potent as morphine. Therefore, any exposure has to be taken seriously. Inadvertent intoxication can occur through small skin cuts, needle sticks or ocular and nasal exposure. Symptoms of exposure include nausea, dizziness, respiratory depression, miosis and quick progression to loss of consciousness, seizures or coma. Anyone working with anaesthetics, particularly in the field, should have a written emergency protocol clearly to identify and determine the steps that should be taken in the event of an exposure. This protocol should be discussed with all participating personnel.
Handling and treatment of accidental exposure to carfentanil or etorphine
Whenever carfentanil or etorphine are used, multiple vials of naloxone should be readily available and kept in date. The exposure kit should also contain: naloxone: 1 mg/mL, 10 mL multidose vials (total 10); five additional vials should be stored in the emergency box. Other items that are essential include: normal saline intravenous fluids, IV administration set, various gauge IV Butterfly catheters, various sized IV catheters and needles, various size syringes (including large sizes for fluid administration), various size gauge needles, tourniquet (used to help establish IV access), alcohol swabs, gauze pads, tape, disposable gloves, pocket mask with one way valve, non-rebreathing mask, SPU resuscitator (AMBU) with reservoir attachment and tubing, carfentanil/etorphine emergency protocol, and drug package inserts. Lastly, a portable oxygen tank should be available whenever potent narcotics are being used.
The protocol for treatment of human narcotic exposure includes:
1.Do not leave the patient unattended!
3.Flush the exposed areas with copious amounts of water or saline. Avoid contamination of additional personnel while doing this
4.Bring the Human Narcotic Exposure Emergency Kit and oxygen to the patient
5.Draw up 30 mL of naloxone (3 bottles, 30 mg total) into a 35 mL syringe
6.Draw up 10 mL of naloxone (1 bottle, 10 mg) into a 12 mL syringe
7.Monitor the patient’s pulse and respiration rate
9.If the patient is awake and talking continue to monitor
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


