Chapter 18 Anesthetic Management
The veterinarian with cattle anesthetic experience will find both anatomic and physiologic similarity with sheep and goats. Physical restraint and local anesthetic techniques are most commonly used to achieve immobility and analgesia for sheep and goats. Pain perception in these animals is no different from that in other species, so analgesia for prevention and easing of pain is an important component of specific veterinary care and general management practices, just as in other animals. Occasionally, general anesthesia is required for surgical intervention. In such instances, balanced anesthetic techniques should be used to provide narcosis, analgesia, and muscle relaxation, thereby minimizing the stress response induced by surgery and anesthesia.
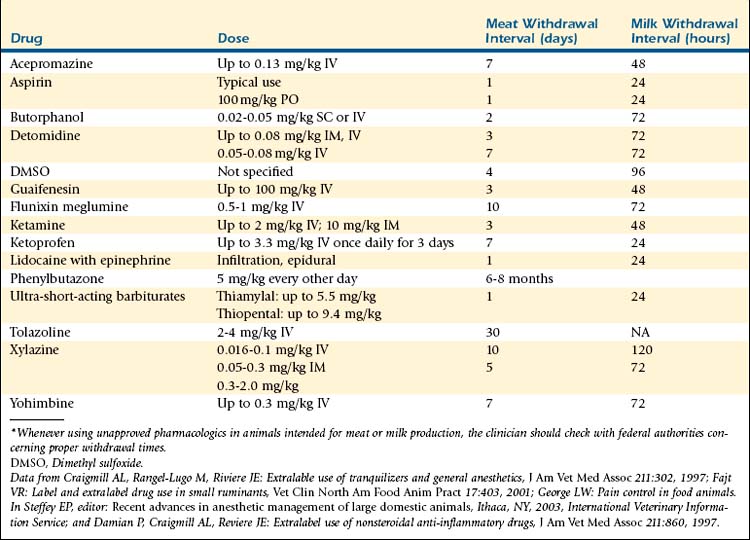
At present, only one anesthetic drug has been approved for use in goats (ophthalmic proparacaine) and only one for use in sheep (thiopental sodium). Extralabel use of drugs is permitted only when animal health is threatened or death may result without treatment. Although issues of violative residues should be considered, use of anesthetics is strictly short term, and animals that have been given such agents are unlikely to be marketed immediately after surgery. Furthermore, anesthetics are administered either intravenously (IV) or by inhalation, and the drugs commonly used today tend to be potent enough that low doses are required to produce general anesthesia. Thus problems with anesthetic drug residues appear to be very rare.1 Table 18-1 summarizes meat and milk withdrawal intervals recommended by the Food Animal Residual Avoidance Databank (FARAD) for some of the analgesics, tranquilizers, and injectable anesthetics typically used in an extralabel manner for sheep and goats.2,3 Clinicians should consult FARAD recommendations whenever using unapproved drugs, because withdrawal times are subject to change.
TABLE 18-1 FARAD Recommended Withdrawal Intervals for Sheep and Goats with Single and Multiple Doses of Anesthetic Drugs*
Preanesthetic Preparation
Domestic ruminants have a multicompartmental stomach with a large rumen that does not empty completely4 and are therefore susceptible to certain complications associated with recumbency and anesthesia. Tympany, bloat, regurgitation, and aspiration pneumonia are common problems that should be anticipated and addressed with the proper precautions. When possible, adult animals should be fasted for 12 to 24 hours and water withheld for 8 to 12 hours before induction of anesthesia. The fasting of neonates is not recommended because of the potential for hypoglycemia in this age group.4 In emergency situations, fasting may not be possible, and precautions should be taken to avoid aspiration of gastric fluid and ingesta. Effective measures include endotracheal intubation and positioning of the animal’s head so that the throat latch area is elevated relative to the mouth and thoracic inlet, which prevents pooling of saliva and ruminal contents in the oral cavity.
Venipuncture and catheterization of the jugular vein usually are performed before induction of anesthesia. A 16-gauge indwelling catheter is appropriate for adult sheep and goats; an 18-gauge catheter is suitable for younger animals. The technique for catheterization in sheep and goats is similar to that used in calves (Figure 18-1).

Intubation is more difficult to accomplish in sheep and goats than in many other animals, for several reasons: The mouth does not open widely, the intermandibular space is narrow, and the laryngeal opening is distant beyond the thick base of the tongue.4 Intubation should be prompt and performed with the animal in sternal recumbency immediately after the induction of anesthesia. Intubation is best accomplished if an assistant pulls the mouth open by means of a loop of gauze placed around the upper jaw and a second loop around the lower jaw and tongue (Figure 18-2). At the same time, the assistant should hyperextend the animal’s neck. If the larynx cannot be visualized, the neck should be extended further.5 A long (25- to 35-cm) laryngoscope blade can be used to suppress the tongue base and epiglottis and enable visualization of the larynx. The next step is placement of a “guide tube” (preferably a 10F, 22-inch-long polyethylene canine urethral catheter that is three times the length of the endotracheal tube), over which the endotracheal tube is slipped into place. This method makes endotracheal intubation much easier to achieve than with other methods (see Figure 18-2). A cuffed endotracheal tube should be used to prevent regurgitation and aspiration of ruminal contents, and the animal should be maintained in sternal recumbency until the cuff is inflated.

Preanesthetics
Preanesthetic tranquilization or sedation is rarely needed in small ruminants. In larger or more vigorous animals, however, the use of a tranquilizer or sedative may minimize the stress caused by forceful restraint, ease the induction process, and decrease the dose requirement for anesthetic, thereby potentially preventing disastrous hypotension (Table 18-2).
TABLE 18-2 Doses of Preanesthetics Commonly Used in Sheep and Goats
| Preanesthetics | Dosage for Sheep | Dosage for Goats |
|---|---|---|
| Atropine | 0.066 mg/kg IV 0.005-0.01 mg/kg SC or IM; 0.02-0.04 mg/kg IV | 0.066 mg/kg IV 0.005-0.01 mg/kg SC or IM; 0.02-0.04 mg/kg IV |
| Glycopyrrolate | 0.002-0.005 mg/kg IV; 0.005-0.01 mg/kg IM 0.01-0.02 mg/kg SC or IM; 0.005-0.01 mg/kg IV | 0.002-0.005 mg/kg IV; 0.005-0.01 mg/kg IM 0.01-0.02 mg/kg SC or IM; 0.005-0.01 mg/kg IV |
| Acepromazine | Less than 50 kg: 0.to 0.2 mg/kg IV More than 50 kg: 0.05-0.1 mg/kg IV or IM 0.05-0.1 mg/kg SC or IM; 0.025-0.05 mg/kg IV 0.04-0.09 mg/kg IM; 0.01-0.02 mg/kg IV | Less than 50 kg: 0.1-0.2 mg/kg IV More than 50 kg: 0.05-0.1 mg/kg IV or IM 0.05-0.1 mg/kg SC or IM; 0.025-0.05 mg/kg IV 0.04-0.09 mg/kg IM; 0.01-0.02 mg/kg IV |
| Chloral hydrate | 30-60 mg/kg IV | 30-60 mg/kg IV |
| Detomidine | 0.001-0.007 mg/kg IV for sedation; 0.04 mg/kg IM, recumbency for 45-60 minutes 0.05-0.08 mg/kg IV | 0.001-0.007 mg/kg IV, sedation; 0.04 mg/kg IM, recumbency for 45-60 minutes 0.05-0.08 mg/kg IV |
| Diazepam | 0.25-0.5 mg/kg IV slowly 0.2-1 mg/kg SC or IM; 0.2-0.4 mg/kg IV | 0.25-0.5 mg/kg IV slowly 0.2-1 mg/kg SC or IM; 0.2-0.4 mg/kg IV |
| Medetomidine | 0.001-0.007 mg/kg IV for sedation; 0.04 mg/kg IM, recumbency for 58 minutes | 0.001-0.007 mg/kg IV, sedation; 0.04 mg/kg IM, recumbency for 58 minutes |
| Midazolam | 0.1-0.5 mg/kg SC, IM, or IV | 0.1-0.5 mg/kg SC, IM, or IV |
| Xylazine | 0.01-0.02 mg/kg IV, standing sedation for 30-60 minutes 0.1-0.2 mg/kg IV, or 0.2-0.3 mg/kg IM, recumbency for 60 minutes 0.1-0.3 mg/kg IV or SC 0.1-0.3 mg/kg SC or IM; 0.025-0.1 mg/kg IV ≤0.1 mg/kg IV; 0.1-0.6 mg/kg IM | 0.01-0.02 mg/kg IV, standing sedation for 30-60 minutes 0.05-0.11 mg/kg IV, or 0.11-0.22 mg/kg IM, recumbency for 60 minutes 0. 1-0.3 mg/kg IV or SC 0.1-0.3 mg/kg SC or IM; 0.05-0.1 mg/kg IV ≤0.1 mg/kg IV; 0.1-0.6 mg/kg IM |
Data from Blaze CA, Glowaski MM, editors: Veterinary anesthesia drug quick reference, St Louis, 2004, Elsevier Saunders; Muir WW, et al, editors: Handbook of veterinary anesthesia, St Louis, 2007, Mosby Elsevier; Cornick-Seahorn JL, editor: The practical veterinarian: veterinary anesthesia, Boston, 2001, Buttorworth Heinemann.
Phenothiazine Derivative
Acepromazine maleate produces mild tranquilization without analgesia. This drug has minimal effects on heart rate and respiratory function. Its use may result in hypotension and increase the risk of regurgitation.6,7 When administering acepromazine, the clinician should avoid using the coccygeal vein for intravenous injection because of the close proximity of the coccygeal artery.6 Prolapse of the penis with the potential for traumatic injury sometimes occurs in sheep and goats after the use of this agent. Furthermore, acepromazine is contraindicated in debilitated or hypovolemic animals.6
α2-Adrenergic Agonists and Antagonists
α2-Adrenergic Agonists
Xylazine hydrochloride probably is the most popular α2-adrenergic agonist in large animal practice today. Ruminants are very sensitive to the effects of xylazine, with goats appearing to be more sensitive than sheep.7 Xylazine is a potent sedative, analgesic, and muscle relaxant that frequently is used as a preanesthetic or anesthetic adjunct in ruminants. Xylazine alone produces dose-dependent effects ranging from standing sedation to full recumbency and immobilization. Xylazine also may cause bradycardia, hypotension, hypoxemia, hypercapnia, pulmonary edema, hyperglycemia, hypoinsulinemia, increased urine production, and an oxytocin-like effect.8 It should be used with extreme caution in animals with preexisting cardiopulmonary disease or urinary tract obstruction. An up to six-fold increase in urine output frequently is observed after xylazine administration.9 Administration of xylazine to ruminants in the final trimester of pregnancy may cause premature parturition and retention of fetal membranes and should therefore be avoided.10 Lateral recumbency has been reported to induce a significant decrease in partial pressure of arterial oxygen (Pao2) in conscious sheep.11 This hypoxemia can occur even when the animal remains standing during xylazine sedation.12,13 Severe hypoxemia and pulmonary edema have been implicated as the causes of death in sheep that die under xylazine anesthesia.14–16 Bronchospasm and venospasm resulting from direct α2-receptor activation on vascular and bronchial smooth muscle, α2 activity–induced transient platelet aggregation with pulmonary microembolism, and release of cytokines and other inflammatory mediators due to α2 activity–induced pulmonary intravascular macrophage activation may be the contributing factors for the development of hypoxemia.17
Epidural administration of xylazine (0.07 to 0.1 mg/kg) with or without lidocaine into the sacrococcygeal space induces long-lasting, good somatic analgesia for open castration in rams (8 hours without lidocaine) and for correction of vaginal prolapse in ewes (24 hours with 0.5 mg/kg of lidocaine).18,19 Visceral analgesia induced by xylazine alone, however, may not be sufficient for ligation of the spermatic cord.18
Detomidine hydrochloride, when administered at an intravenous dose of 0.02 mg/kg, produces sedation comparable to that provided by 0.04 mg/kg of xylazine.20 Increasing the dose to 0.03 mg/kg, which is equivalent to 0.15 mg/kg of xylazine and 0.01 mg/kg of medetomidine, induces recumbency in sheep.21 The pharmacologic effects of detomidine are very similar to those of xylazine.21 Hypoxemia and pulmonary edema may occur with all α2-agonists, but the degree of severity of hypoxemia is reported to be less with detomidine.17 In addition, ruminants appear to be less sensitive to detomidine than to xylazine. Unlike xylazine, detomidine at intravenous doses smaller than 0.04 mg/kg does not produce an oxytocin-like effect on the uterus in gravid cattle. Even though detomidine at doses higher than 0.04 mg/kg may increase the electrical activity of the uterine muscles, it does not induce the synchronization of the bursts of potentials that is characteristic of parturition. Detomidine is unlikely to induce abortion in pregnant ruminants at therapeutic doses22,23 and therefore may be safer for pregnant sheep and goats.
Medetomidine hydrochloride in doses of 0.001 to 0.007 mg/kg IV induces dose-dependent sedation and analgesia: 0.005 mg/kg appears to produce analgesia in sheep comparable to that provided by 0.015 mg/kg of fentanyl.24 At an intramuscular dose of 0.04 mg/kg, medetomidine induces recumbency for 58 minutes, as well as good analgesia and marked muscle relaxation for 30 to 45 minutes. Sheep usually recover within 1.5 to 2 hours after regaining the righting reflex.25 When medetomidine was administered intramuscularly (IM) as a preanesthetic at either of two doses (0.005 or 0.01 mg/kg) 30 minutes before induction with propofol and maintenance with isoflurane, medetomidine at either dose induced decreases in heart rate and respiratory rate. Mean arterial blood pressure values were significantly higher in sheep receiving a higher dose of medetomidine than in those receiving a lower dose or no preanesthetic medetomidine. In general, the administration of medetomidine reduced the dose requirement of propofol for induction and isoflurane anesthesia during surgery.26 In sheep anesthetized with medetomidine (0.02 mg/kg IV) and ketamine (2 mg/kg IV) and breathing room air, Pao2, arterial pH, and arterial oxygen (O2) saturation decrease and the partial pressure of arterial carbon dioxide (Paco2) increases significantly. Supplementation of 100% O2 may improve Pao2 and hemoglobin saturation.27
α2-Adrenergic Antagonists
The pharmacologic effects induced by xylazine, detomidine, or medetomidine can be effectively antagonized by an α2-adrenergic antagonist such as yohimbine, tolazoline, or atipamezole (Table 18-3). These antagonists can be used to shorten recovery time and prevent the significant adverse effects sometimes seen with agonists, especially accidental overdose. However, these drugs are not without risks: The death of a sheep after administration of a large dose of yohimbine (0.8 mg/kg IV) has been reported.28 For administration of an antagonist, slow injection is recommended to avoid sudden awareness of pain and excitement on the part of the animal. Rapid injection of tolazoline has been reported to cause significant cardiac stimulation, tachycardia, increased cardiac output, vasodilation, coronary vasodilation, and gastrointestinal distress.29 Ruminants and camelids apparently are more sensitive to tolazoline than other species, and death has been reported in several animals after its use.30,31 When administered alone to Holstein calves, intravenous tolazoline caused coughing, increased frequency of defecation, and a mild increase in breathing effort at a dose of 1.5 mg/kg. At higher doses (2 to 10 mg/kg IV), adverse effects such as bright red conjunctival mucous membranes, coughing, nasal discharge, salivation, increased breathing effort (labored breathing), CNS depression, signs of abdominal pain, straining, head pressing, restlessness, and increased frequency of defecation to severe diarrhea were observed. Nonetheless, all calves in the study recovered uneventfully.31 Therefore lower doses at 0.5 to 1.5 mg/kg IV are now recommended in ruminants including sheep and goats. When atipamezole (0.1 mg/kg IV) was administered to six goats to antagonize medetomidine (0.02 mg/kg IV)-induced sedation and recumbency, all goats stood within 86 ± 24 seconds. Four goats developed piloerection, and all six appeared to be agitated and vocalized.32 Nevertheless, the undesirable effects of α2-antagonists are extremely rare in healthy animals when the drugs are administered by slow intravenous injection and at appropriate dosages.
TABLE 18-3 Doses of Antagonists Commonly Used in Sheep and Goats
| Drug | Dosage for Sheep | Dosage for Goats |
|---|---|---|
| α2-ADRENERGIC ANTAGONIST | ||
| Atipamezole | 0.05 mg/kg IV 0.125-0.2 mg/kg slow IV | 0.05 mg/kg IV 0.125-0.2 mg/kg slow IV |
| Tolazoline | 2 mg/kg slow IV 0.5-1.5 mg/kg slow, IV | 2 mg/kg slow IV 0.5-1.5 mg/kg slow, IV |
| Yohimbine Yohimbine Yohimbine Yohimbine | 0.125-0.22 mg/kg slow IV 0.1-0.3 mg/kg IV 1, IV 0.3-0.5 mg/kg IM | 0.125-0.22 mg/kg slow IV 0.1-0.3 mg/kg IV 0.3-0.5 mg/kg IM |
| BENZODIAZEPINE ANTAGONIST | ||
| Flumazenil | 0.1-1 mg/kg IV | 0.1-1 mg/kg IV |
| NEUROMUSCULAR BLOCKING DRUG ANTAGONIST | ||
| Edrophonium | 0.5 mg/kg IV | 0.5 mg/kg IV |
| Neostigmine | 0.02-0.04 mg/kg IV | 0.02-0.04 mg/kg IV |
| Pyridostigmine | 0.2 mg/kg IV | 0.2 mg/kg IV |
| NONSPECIFIC ANTAGONIST | ||
| Doxapram Doxapram | 5-10 mg/kg IV 0.2-0.4 mg/kg IV | 5-10 mg/kg IV |
| OPIATE ANTAGONIST | ||
| Nalmefene | 0.25-30 μg/kg IV | 0.25-30 μg/kg IV |
| Naloxone | 0.01-0.02 mg/kg IV, titrate to effect | 0.01-0.02 mg/kg IV, titrate to effect |
| Naltrexone | 0.05-0.1 mg/kg SC | 0.05-0.1 mg/kg SC |
Data from Blaze CA, Glowaski MM, editors: Veterinary anesthesia drug quick reference, St Louis, 2004, Elsevier Saunders; Muir WW, et al, editors: Handbook of veterinary anesthesia, St Louis, 2007, Mosby Elsevier; and Cornick-Seahorn JL, editor: The practical veterinarian: veterinary anesthesia, Boston, 2001, Butterworth Heinemann.
Benzodiazepines
Diazepam has a mild sedative-hypnotic effect and produces decreased anxiety along with muscle relaxation. Diazepam often is used for its anxiolytic effect in high-risk animals because of its minimal cardiovascular and pulmonary effects at therapeutic doses. It also can be used in combination with ketamine to improve muscle relaxation during anesthesia.33
In goats, intramuscular midazolam (0.6 mg/kg) induced ~20 minutes of sedation. Hypnosis with recumbency for 10 to 20 minutes occurred with intravenous administration of midazolam at 0.6 and 1.2 mg/kg. Increasing the dose to 1.2 mg/kg increased the degree of reflex suppression and the animals appeared to be in a light plane of anesthesia, as evidenced by the lack of response to mechanical stimulation applied by tail base clamp.34
Anesthetics (Table 18-4)
Injectable Anesthetics
Thiopental sodium can be used to induce anesthesia in sheep and goats; the depth of anesthesia and muscle relaxation is sufficient for endotracheal intubation. Additional incremental doses may be administered to prolong anesthesia.4 A guaifenesin-thiopental mixture can be administered to effect, to induce and maintain short-term anesthesia. The final concentration of the mixture is 5% (50 mg/mL) guaifenesin and 0.2% (2 mg/mL) thiopental.35 Thiopental causes minimal cardiovascular depression. A moderate tachycardia, slight decrease in mean arterial blood pressure, and short-lived respiratory depression usually occur immediately after rapid induction of anesthesia with thiopental. Transient apnea is not uncommon during induction with thiopental, and spontaneous breathing returns within several minutes. With prolonged apnea, the animal should be intubated and ventilated until spontaneous breathing resumes.36 Recovery from thiopental anesthesia relies mainly on redistribution of the drug from the brain to the peripheral tissues. Administration of a large dose or prolonged infusion may result in extremely prolonged recovery. Therefore maintenance of anesthesia with thiopental is not recommended if the surgical procedure will require more than 1 hour.36
TABLE 18-4 Doses of General Anesthetics Commonly Used in Sheep and Goats
| Anesthetic Agent(s) | Dosage for Sheep | Dosage for Goats |
|---|---|---|
| Guaifenesin | 30-90 mg/kg IV; when muscle relaxed, followed by ketamine 1.1 mg/kg IV | 30-90 mg/kg IV; when muscle relaxed, followed by ketamine 1.1 mg/kg IV |
| Atracurium (neuromuscular blocking drug) | 0.2 IV mg/kg for initial dose; 0.1 IV mg/kg for repeat dose 0.005/mg/kg/hour IV (infusion) | 0.2 IV mg/kg for initial dose; 0.1 IV mg/kg for repeat dose 0.005/mg/kg/hour IV (infusion) |
| Etomidate | 0.5-1 mg/kg IV | 5-10 mg/kg IV |
| Ketamine | 22 mg/kg SC or IM; 2-4 mg/kg IV | 11 mg/kg SC or IM; 2-4 mg/kg IV |
| Acepromazine Ketamine | 0.55 mg/kg IV 2.2 mg/kg IV | N/A |
| Diazepam Ketamine Diazepam Ketamine Diazepam Ketamine | 0.11 mg/kg IV 4.4 mg/kg IV 0.25-0.5 mg/kg IV 4-7.5 mg/kg IV 0.28 mg/kg IV 5.5 mg/kg IV | 0.11 mg/kg IV 4.4 mg/kg IV 0.28 mg/kg IV 5.5 mg/kg IV |
| Guaifenesin (5%) plus ketamine (0.1%) | Induction: 2 mL/kg IV, 50-75% calculated dose first Maintenance: 2.2 mL/kg/hour or to effect | Induction: 2 mL/kg IV, 50-75% calculated dose first Maintenance: 2.2 mL/kg/hour or to effect |
| Medetomidine Ketamine Medetomidine Ketamine | 0.02 mg/kg IV 2 mg/kg IV 0.02 mg/kg IV 0.5-1 mg/kg IV | 0.02 mg/kg IV 2 mg/kg IV 0.02 mg/kg IV 0.5-1 mg/kg IV |
| Xylazine Ketamine Xylazine Ketamine | 0.22 mg/kg IM; wait 10 minutes 10-15 mg/kg IM 0.03-0.2 mg/kg IV or IM 5 mg/kg IV | 0.22 mg/kg IM; wait 10 minutes 11 mg/kg IM 0.03-0.2 mg/kg IV or IM 5 mg/kg IV |
| Guaifenesin (5%), xylazine (0.01%), and ketamine (0.1-0.2%) Guaifenesin (5%), xylazine (0.005%), and ketamine (0.1-0.2%) | Induction: 0.67-1.1 mL/kg Maintenance: 2.2 mL/kg/hour to effect Induction: 0.5-1 mL/kg Maintenance: 1.5-2 mL/kg/hour | Induction: 0.67-1.1 mL/kg Maintenance: 2.2 mL/kg/hour to effect Induction: 0.5-1 mL/kg Maintenance: 1.5-2 mL/kg/hour |
| Pancuronium (neuromuscular blocking drug) | 0.005 mg/kg IV | 0.005 mg/kg IV |
| Propofol | Induction: 3-4 mg/kg IV or 4-8 mg/kg IV Maintenance: 18-40 mg/kg/hour IV (infusion) or to effect 4-6 mg/kg IV | Preanesthetic: detomidine 0.01 mg/kg IM plus butorphanol 0.1 mg/kg IM Induction: 3-5 mg/kg IM Maintenance: 31 mg/kg/hour 4-6 mg/kg IV |
| Diazepam Propofol | 0.28 mg/kg IV 4-6 mg/kg IV | 0.28 mg/kg IV 4-6 mg/kg IV |
| Thiopental | 10-16 mg/kg IV | 10-16 mg/kg IV |
| Guaifenesin (5%) plus thiopental (0.2%) | Induction: 2 mL/kg IV, 50-75% calculated dose first Maintenance: 2.2 mL/kg/hour or to effect | Induction: 2 mL/kg IV, 50-75% calculated dose first Maintenance: 2 mL/kg/hour or to effect |
| Tiletamine plus zolazepam (Telazol) | 2-6 mg/kg IM; 1-4 mg/kg IV 5.5 mg/kg IV, anesthesia for 100 minutes 5.5 mg/kg IV with butorphanol 0.1 mg/kg IV, anesthesia for 100 minutes | 2-6 mg/kg IM; 1-4 mg/kg IV 5.5 mg/kg IV, anesthesia for 100 minutes 5.5 mg/kg IV with butorphanol 0.1 mg/kg IV, anesthesia for 100 minutes |
| Xylazine Telazol | 0.05-0.1 mg/kg IV or IM 2-4 mg/kg IV or IM | 0.05-0.1 mg/kg IV or IM 2-4 mg/kg IV or IM |
| Vecuronium (neuromuscular blocking drug) | 0.005 mg/kg IV | 0.005 mg/kg IV |
Data from Blaze CA, Glowaski MM, editors: Veterinary anesthesia drug quick reference, St Louis, 2004, Elsevier Saunders; Muir WW, et al, editors, Handbook of veterinary anesthesia, St Louis, 2007. Mosby Elsevier; and Cornick-Seahorn JL, editor: The practical veterinarian: veterinary anesthesia, Boston, 2001, Butterworth Heinemann.
Ketamine hydrochloride, a dissociative derivative, probably is the most commonly used injectable anesthetic in sheep and goats. Acepromazine, diazepam, xylazine, and medetomidine can be used in combination with ketamine to enhance the degree of analgesia and muscle relaxation during anesthesia. Unlike other conventional anesthetics, ketamine does not depress cardiovascular function; instead, heart rate and arterial blood pressure increase during ketamine anesthesia as a result of central sympathetic stimulation. A mixture of ketamine (1 mg/mL) and guaifenesin can be used to maintain short-term anesthesia.37 A combination of guaifenesin (50 mg/mL), ketamine (1 to 2 mg/mL), and xylazine (0.1 mg/mL) (GKX), often referred to as “triple drip,” can be used for both induction and maintenance of anesthesia.38
Telazol (Pfizer Animal Health, New York) is a proprietary combination of tiletamine (dissociative) and zolazepam (benzodiazepine) in a 1:1 (weight-weight) ratio. Compared with ketamine, Telazol produces better muscle relaxation, more profound analgesia, and longer-lasting effects. In ruminants the induction of anesthesia after Telazol administration is rapid and smooth, and the recovery usually is gradual and prolonged.16 Similar to ketamine, this drug causes cardiovascular stimulation rather than depression.37 Hypoventilation and hypothermia may occur during Telazol-induced anesthesia. Assisted or controlled ventilation with O2 supplementation may be required in cases of severe hypoventilation and hypoxemia. Animals should be placed in sternal recumbency with support throughout the recovery period.16
Propofol is a unique short-acting anesthetic. Structurally, this drug does not relate to any of the injectable anesthetics currently available in veterinary practice. Propofol is only slightly water-soluble and is formulated as an emulsion containing 10 mg of propofol, 100 mg of soybean oil, 22.5 mg of glycerol, and 12 mg/mL of egg lecithin in sterile glass ampules. Because this emulsion contains no preservative, after the ampule is opened, the contents should be used or discarded within 8 hours.37 A single dose of propofol (2 mg/kg) induces approximately 10 minutes of anesthesia, with complete recovery occurring in 20 to 30 minutes.4,39 Propofol is best used for induction before inhalation anesthesia; it also can be given as a continuous infusion to maintain short-term anesthesia.40–42 In goats, a combination of detomidine, butorphanol, and propofol for induction and continuous intravenous infusion of propofol for maintenance provides adequate anesthesia for castration or ovariectomy.43
A comparative study was performed to evaluate use of propofol (3 mg/kg IV), thiopental (8 mg/kg IV), and ketamine (10 mg/kg IV) as induction agents before halothane anesthesia in goats. The result of this study indicated that propofol was superior to thiopental or ketamine as an induction agent owing to rapid and uneventful recovery from its effects. Time to standing with propofol after 30 minutes of halothane anesthesia was 18 ± 2.4 minutes, as opposed to 43.9 ± 7.3 minutes with thiopental and 76.9 ± 10.3 minutes with ketamine.44
Total intravenous anesthesia (TIVA) with ketamine and propofol infusion has been used to maintain immobilization and anesthesia in goats undergoing magnetic resonance imaging (MRI) procedure. These goats were sedated with midazolam (0.4 mg/kg IV), and anesthesia was induced with intravenous propofol (1 mg/kg) and ketamine (3 mg/kg) and maintained with constant infusion rates of propofol (0.3 mg/kg/minute) and ketamine (0.03 mg/kg/minute) with or without sevoflurane. Goats anesthetized with propofol and ketamine exhibited significant decreases in respiratory rates and increases in arterial blood pressure values. As supported by our own experience, overall, anesthesia with ketamine and propofol infusion is practical and safe for animals undergoing MRI procedures.45
Inhalation Anesthetics
Inhalation anesthetics require expensive and specialized equipment for delivery to the patient. However, these agents allow veterinarians to perform complicated and prolonged surgery. Either halothane or isoflurane can be used effectively and safely in sheep and goats. Mask induction may not be a wise choice in healthy adults but can be used in smaller or debilitated animals. Use of a small animal anesthesia machine with a double carbon dioxide (CO2)-absorbent canister usually is adequate for most sheep and goats. The clinician should be aware of a rare condition called halothane-induced hepatitis, an acute, massive liver necrosis that sometimes occurs after halothane anesthesia in healthy goats, especially after prolonged exposure.46,47 Clinical signs, including depression, inappetence, salivation, teeth grinding, head pressing, and icterus, usually appear within 24 hours. Serum concentrations of aspartate transaminase, bilirubin, alkaline phosphatase, and creatinine and blood urea nitrogen are significantly increased from normal ranges. Death usually occurs within 4 days, and histopathologic examination reveals centrilobular necrosis. Necrosis of the proximal renal tubules, abomasal ulceration, and hepatic encephalopathy have been observed in some cases.46,47 Severe hypotension, hypoxemia, and hepatic hypoxia may encourage the reductive metabolism of halothane, leading to the production of toxic free radicals.48 Therefore maintaining adequate cardiovascular function and oxygenation through careful monitoring and supportive therapies is key to a successful anesthetic procedure.
Isoflurane and sevoflurane have become popular inhalation anesthetics in recent years. Both anesthetics have lower potency (halothane: 0.96%; isoflurane: 1.29%; sevoflurane: 2.33%)49 and lower lipid solubility compared with halothane (halothane: 2.36; isoflurane: 1.41; sevoflurane: 0.69).50 Thus the induction of anesthesia and recovery usually occur more rapidly with these agents than with halothane. Hepatitis associated with halothane is unlikely to develop with isoflurane and sevoflurane owing to the fact that elimination of these two anesthetics involves very little hepatic metabolism (halothane: 20%; isoflurane: 0.25%; sevoflurane: 3% to 5%).50 Isoflurane and sevoflurane have similar cardiovascular and pulmonary effects, which include vasodilation and dose-dependent decreases in arterial blood pressures, respiratory rate, tidal volume, and minute ventilation. Decreases in arterial blood pressure during halothane anesthesia have been shown to be the result of depression of myocardial contractility and the subsequent decrease in cardiac output. In contrast with halothane, the vasodilating effect of isoflurane and sevoflurane is believed to be the primary contributing factor in the decreases in arterial blood pressure.49
Local Anesthetics
Local anesthetics produce their effects by blocking the propagation of action potentials along nerve axons in a reversible manner. These anesthetics can be injected into the tissue at the surgical site to produce local anesthesia, or they can be administered in the perineural area of major nerves to produce regional anesthesia (see Chapter 8). In small ruminants, many surgical procedures are performed safely and painlessly with the use of local or regional anesthesia.
All local anesthetics have similar physical properties and molecular structures. Most of them are weakly basic tertiary amines with a hydrophilic end, a lipophilic end, and an intermediate hydrocarbon chain. They are generally available as acid solutions of the water-soluble salts. The acid salt is neutralized in the tissue, liberating the base, which then penetrates the cell membrane and interrupts the propagation of the action potential. This mechanism of action means that a local anesthetic is less effective in inflamed tissue with lower pH, because less liberation of the basic form of the drug occurs under these conditions.51 Local anesthetics are classified as either ester-link or amide-link drugs, depending on the intermediate chain structure. Inactivation of ester-link local anesthetics (e.g., procaine, tetracaine) depends on hydrolysis by cholinesterase enzymes in the plasma and to a lesser extent in the liver. Metabolism of amide-link local anesthetics (e.g., lidocaine, bupivacaine, mepivacaine) relies on microsomal enzymes located primarily in the liver.51
Lidocaine probably is the most popular local anesthetic used and may produce anesthesia for 0.75 to 2 hours. Because of its ability to induce vasoconstriction in the tissue around the injected area, epinephrine decreases systemic absorption of concurrently administered local anesthetics. Therefore epinephrine (1:200,000 to 1:50,000) at concentrations of 5 to 20 μg/mL can be incorporated with or added to lidocaine solution to prolong the duration of local anesthesia.52 Mepivacaine (5 mg/kg), with effect duration of 1.5 to 3 hours, and bupivacaine (2 mg/kg), with effect duration of 4 to 8 hours, can be used for procedures that require a longer duration of local anesthesia.51,53 Administration of a large single dose or repeated small doses of local anesthetics can result in toxicity in sheep and goats, especially in neonatal and young patients. Clinical signs of toxicity include nystagmus, muscle fasciculation, CNS stimulation progressing to opisthotonos and convulsions, hypotension, respiratory arrest, and circulatory collapse, with death in some cases.51 The maximum calculated safe dose of lidocaine was reported to be 13 mg/kg in one study.54 In another study, accumulated intravenous doses of 5.8 mg/kg, 18 mg/kg, and 42 mg/kg induced signs of toxicity in adult, neonatal, and fetal sheep, respectively.55 Intravenous infusion of mepivacaine in sheep induced convulsions at doses of 7.5 to 7.9 mg/kg and cardiovascular collapse at doses as high as 52 to 69 mg/kg.56 Bupivacaine is approximately four times more potent than lidocaine, so a 0.5% solution produces the same degree of neuronal blockade as that achieved with a 2% lidocaine solution.57
Ewing58 suggests using a maximum of 6 mg/kg of lidocaine or mepivacaine and 2 mg/kg of bupivacaine in small ruminants. With this maximum safe dose in mind, the clinician should dilute lidocaine and mepivacaine solutions to 1% and 0.5%, respectively, to prevent overdosage when using these drugs in lambs and kids.58 Diazepam (0.1 mg/kg IV) or thiopental (5 mg/kg IV) should be administered if seizure activity or convulsions caused by accidental overdose persist longer than 1 to 2 minutes.57,59
Perioperative Management And Recovery
Monitoring During Anesthesia
Arterial hemoglobin O2 saturation is measured by pulse oximetry with the sensor clip placed on the lingual artery in the tongue or on the auricular artery in an ear. Normal arterial hemoglobin O2 saturation should always be close to 98% to 100%. Indirect arterial blood pressures can be measured by an oscillometric blood pressure machine with an inflatable pressure cuff placed on the tail or mid thigh and over the coccygeal or dorsal metatarsal artery, respectively. Normal values for heart rate, respiratory rate, arterial blood pressures and various arterial blood gases are listed in Table 18-5.
TABLE 18-5 Normal Vital Signs and Values for Anesthetized Sheep and Goats
| Vital Sign or Value | Values for Sheep and Goats |
|---|---|
| Heart rate (beats/min) | 80-150 |
| Respiratory rate (breaths/min) | 20-40. |
| Systolic arterial pressure (mm Hg) | 80-120. |
| Mean arterial pressure (mm Hg) | 75-100. |
| Diastolic arterial pressure (mm Hg) | 60-80. |
| Partial pressure of arterial carbon dioxide (Paco2) (mm Hg) | 28-36. |
| Partial pressure of arterial oxygen (Pao2) (mm Hg) | 72-90 |
| Arterial pH | 7.48-7.58. |
Data from Riebold TW, Geiser DR, Goble DO: Clinical techniques for food animals anesthesia. In Riebold TW, Geiser DR, Goble DO, editors: Large animal anesthesia: principles and techniques, ed 2, Ames, Iowa, 1995, Iowa State University Press; and Alon E, et al: Effects of propofol and thiopental on maternal and fetal cardiovascular and acid-base variables in the pregnant ewes, Anesthesiology 78:562, 1993.
Sheep and goats usually recover from anesthesia gradually and smoothly. Emergence delirium and premature attempts to stand seldom occur in these animals. They should be placed in sternal recumbency with support, if necessary, during the recovery period. If regurgitation occurred during anesthesia, the oral cavity and pharynx should be lavaged to prevent aspiration of ruminal materials and subsequent aspiration pneumonia. The endotracheal tube should be left in place until the animal regains its chewing and coughing reflexes. This tube should be removed with the cuff inflated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


