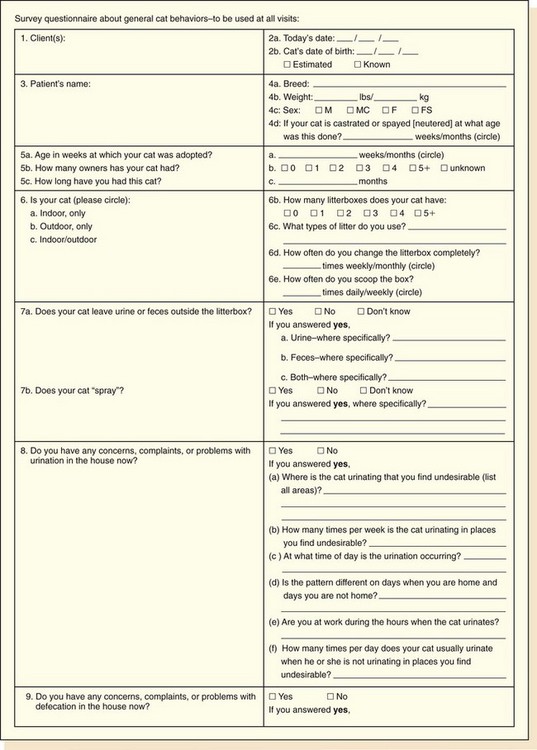
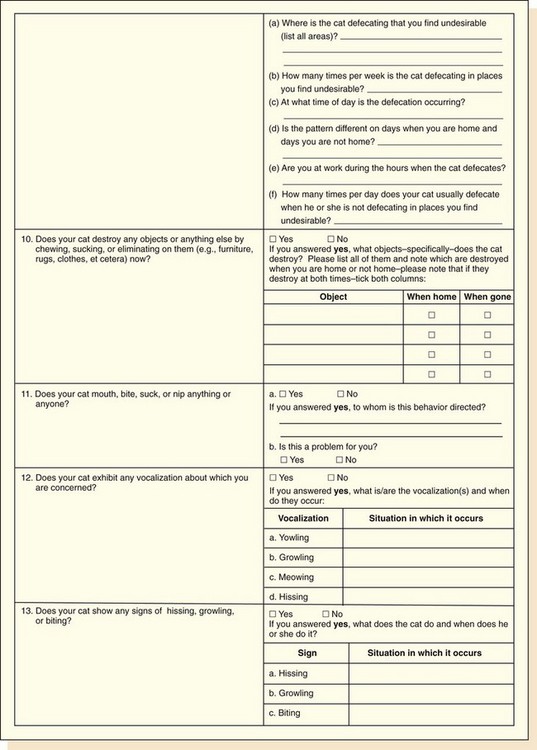
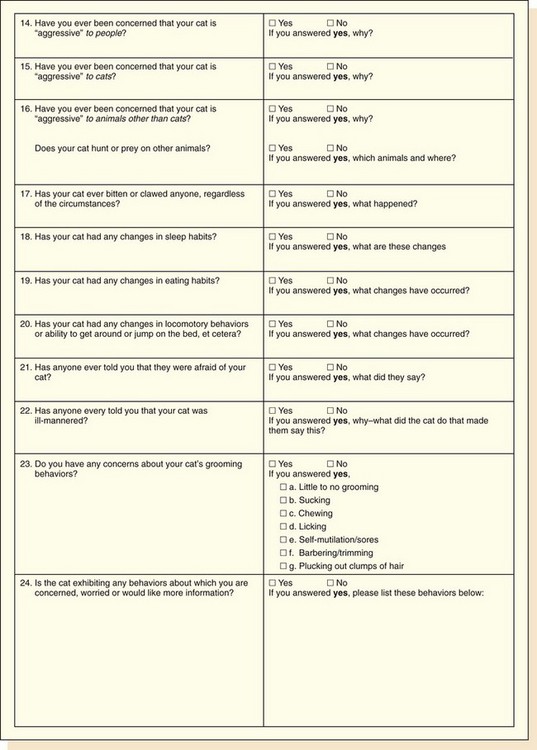
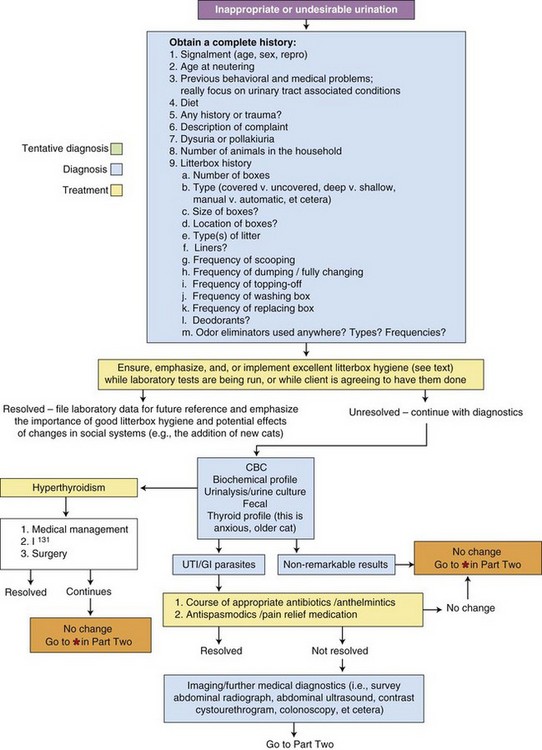
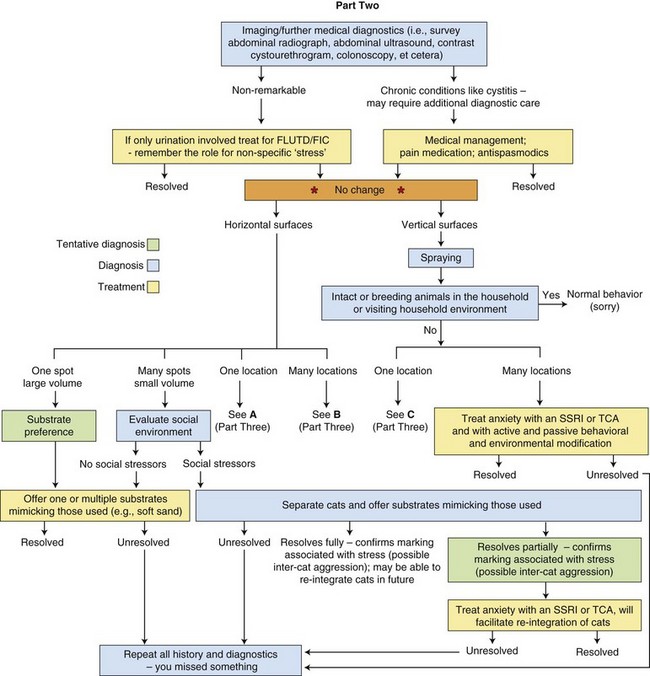
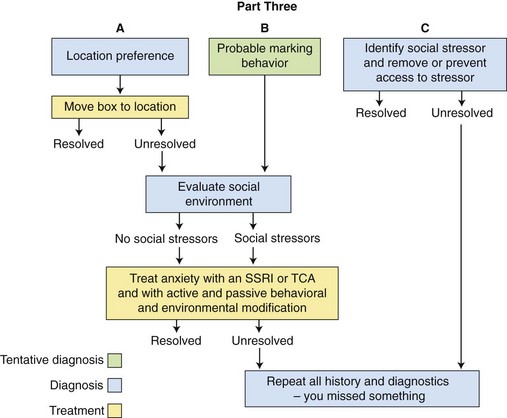
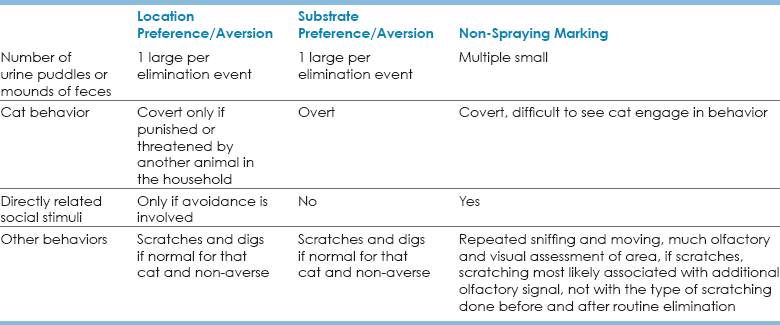
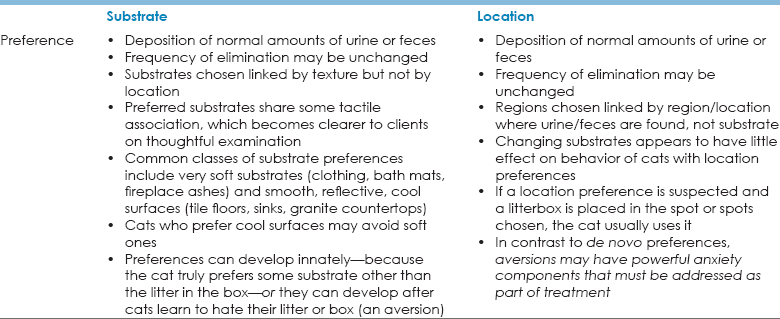
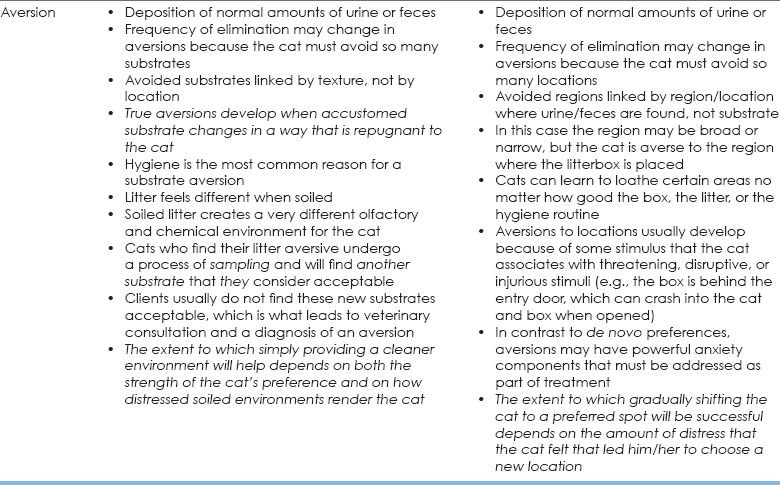
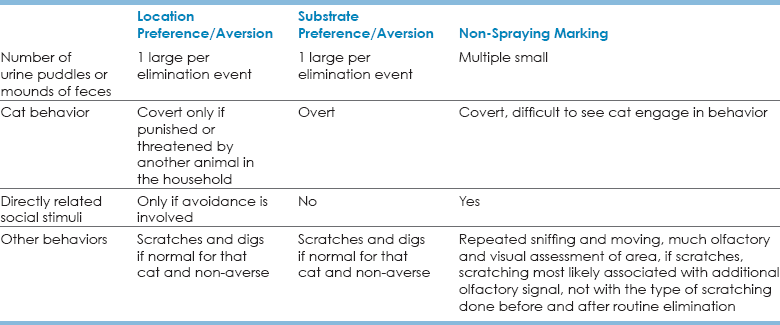
Chapter 9 • Dogs, as a species separate from wolves, likely co-evolved with humans over thousands or tens of thousands of years, during which time they may not have been fully “domesticated.” • “Domestication” may have occurred when we began to develop breed groups intended for specific tasks, which happened 3000 or more years ago. In contrast to wolves, which require handling by humans early in their ontogeny (beginning by at least 14 days of age) if they are not to be fearful and reactive to humans, most dogs can adapt to delays in handling and exposure, and their normal, innate sensitive periods are greatly expanded from those of wolves. When dogs cannot adapt or when they seem to have short sensitive periods, such patterns are indicative of pathology. • In dogs, it is likely that this sensitive period expansion occurred concomitantly with changes in molecular and neurochemical function and gene expression (Saetre et al., 2004), which may represent some of the true outcomes of active “domestication.” In contrast to dogs but similar to other, non-domesticated species, cats have a relatively short and truncated sensitive period for exposure to humans (Karsh, 1983a, 1984), which may be associated with or evidence of lack of tampering associated with “domestication.” Combined with a remarkable neurology that allows for extremely rapid and pronounced arousal and reactivity (discussed later), this shortened sensitive period of cats may suggest why true domestication may be only ongoing now, while also shedding light on the potential etiology of some common feline behavioral patterns and pathologies (i.e., inter-cat aggression, impulse-control aggression, re-directed aggression). • We have not selected cats to “please” us or to be easily handled by us, attributes that Galton (1865) stated were necessary for successful domestication to occur (see Chapter 8). No cat has been selected to work actively with us in a collaborative partnership, and although we lack extensive global data, the sensitive periods of cats who have been housecats for generations do not seem to differ from cats who have been free-ranging or feral for generations. Because of how cats may become feral, there may also be contributory genetic factors that influence the heritability of fear, which may influence how effects of social exposure are manifest or mitigated. There is scant research on this topic, but the implications for behaviors and interactions with humans are profound. • Domestic cats have traditionally been defined as “sit-and-wait” predators, meaning that they hide from their prey and sit and wait by trails, dens, nests, et cetera, as indicated by physical, olfactory, and vocal cues about prey activity. Among mammals, cats are really the only “sit-and-wait” predators, and domestic cats are the quintessential mammalian species using this strategy. Coat color patterns in ancestral cats and many extant cat types/breeds act as disruptive coloration and aid the cat in hiding. As a condition of the “sit-and-wait” hunting strategy, cats are compelled to sit quietly hidden and then react almost instantly with a heightened level of arousal. The behavioral and neurochemical difference between sitting quietly hidden and the profound arousal and reactivity required for successful hunting may have placed constraints on feline brain development with respect to cognitive and social strategies. Cats have “normal” arousal patterns that are different from other species, an observation that likely has implications for how they develop problematic or pathological behaviors. • As we have moved with cats to more urban lifestyles many of the behaviors that are normal for cats could be and frequently are problematic for their humans (i.e., eliminating and digging in gardens, especially if those gardens belong to others). • Behaviors that people might find distressing (e.g., hiding, spraying, fighting with another cat) may be a fairly normal cat’s response to an environment that is confusing, stressful, or distressing to the cat. • Left to themselves, cats range widely. When they are constrained to live within a house or an apartment, that spatial constraint may alter and/or intensify a number of behaviors other than behaviors associated with mobility. • We have no idea how often we see the types of extreme behavioral pathologies in “domestic” cats that we now know appear endogenously in dogs. We do know that when such profoundly abnormal behavior reaches the level of true pathology, as is the case in feline obsessive-compulsive disorder (OCD), the manifestation of the condition always appears to have a component of environmental change or disruption. In other words, although it is possible that the cat may be exhibiting pathological OCD (or other truly abnormal behaviors) at some very low level, and/or the cat may have a risk/liability to develop OCD, the abnormality is not seen or fully manifest until the additional social or environmental stressor is supplied (Overall and Dunham, 2002). That the intersection of innate feline reactivity with other social/physical environments so consistently seems to be involved in some aspect of pathology may be further evidence that cats have not yet been “domesticated.” • Each year in the United States, 22,000 cases (1.8 to 10 cases/100,000 people) of CSD have historically been reported. There have been 2,200 people hospitalized annually (Jackson et al., 1993). • The presumptive agent in CSD is the rickettsial organism, Bartonella (formerly Rochalimaea) hensalae. An occasional contributory role has been postulated for the bacteria Afipia felis. Of 45 human patients with CSD, 38 had titers of at least 1 : 64 for B. hensalae. B. hensalae is likely the predominant, but not the only, cause of CSD, and other Bartonella species have been implicated in infection (Breitschwerdt, 2011). • CSD is most commonly seen in the late summer and fall everywhere it has been studied and coincides with seasonality in births of kittens (spring) and the entry of these kittens into the house in the fall/winter (Sanguinetti-Morelli et al., 2011). • Flea infestations may be associated with a higher incidence of Bartonella infections, and it has been reported that most human patients with CSD have at least one kitten that has fleas (Zangwill et al., 1993). Patients with CSD are more likely to have a kitten 1 year of age or younger or to have been scratched by a kitten, than are non-patients (Zangwill et al., 1993). Although human patients diagnosed with CSD and living in households with kittens are more likely to have been scratched or bitten than humans living in households without kittens, there appears to be no association, other than age, with patients’ cats and cats of controls when indoor/outdoor status, litterbox use, and hunting behaviors are examined (Zangwill et al., 1993). • Infection with Bartonella can occur without any history of bites or scratches by cats or exposure to cats. Coupled with the extremely complex relationship that the Bartonella organism has with vectors and reservoir hosts, it is not surprising that feline bartonellosis need not always manifest in the same manner across patients (Breitschwerdt, 2008). • Cats transmitting Bartonella appear healthy, although they may have long-lasting, active B. hensalae infections (Regnery et al., 1992). People with what is viewed as traditionally conceived CSD tend to have localized skin lesions and regional lymph node involvement 3 weeks after exposure. Lymph nodes remain enlarged for several months. Systemic illness is rare, but fever, headache, splenomegaly, and malaise are common. These symptoms are usually self-resolving; however, arthritis, neuroretinitis, pleurisy, pneumonia, osteolytic lesions, granulomatous hepatitis, and encephalitis with coma and seizure can be unusual sequelae (Tompkins and Steigbigel, 1993). Individuals with immunocompromise or immunosuppression are at risk for more severe disease. Treatment ranges from outpatient care comprising relatively short courses of antibiotics to detailed, extended inpatient care. • Bartonella species infections are increasingly implicated as a potential contributory factor in many immune diseases, including rheumatoid arthritis, and in vector-mediated chronic bacteremias (Maggi et al., 2012). • T. gondii oocytes are shed in feces. • Because cats are the final host and reservoir for T. gondii, cats are blamed for human infection. However, humans likely contact T. gondii most frequently through exposure to raw meat that has been infected because of poor hygiene (Torda, 2001). • Human infection is rare and usually asymptomatic, unless the human is pregnant or immunosuppressed. • Pregnant woman can pass T. gondii to the fetus during pregnancy, resulting in abortion, stillbirth, or neurological complications for the infant (Tenter et al., 2000). • Immunosuppressed individuals may develop fulminant forms of the disease. • Pregnant and immunosuppressed humans should not handle raw meat, cat feces, or cat litter; should cook all meat thoroughly to ensure that cysts are killed before consumption; and should wash their hands thoroughly after interacting with their cats. • Information for clients is available on the following websites: www.petsandparasites.org./cat-owners and www.cdc.gov/parasites/toxoplasmosis/gen_info/pregnant.html (both accessed April 24, 2012). • Toxocariasis is a zoonosis caused by accidental human ingestion of the embryonated eggs of the roundworms Toxocara canis and Toxocara cati, which routinely affect dogs and cats. • Especially in urban areas, cats with large—and likely untreated—worm burdens may use the same sandboxes and grassy areas in which human children play as areas to eliminate. • If children ingest the eggs, the larvae hatch and migrate through the lungs and liver, causing inflammatory responses and clinical signs (visceral larval migrans), and/or the nervous system, potentially becoming stranded in the eye (ocular larval migrans) and causing blindness. • Cats and dogs should be controlled in public spaces, and their feces should be picked up and disposed of hygienically. Children playing in public parks should be encouraged to wash their hands frequently. Clean water and cleansing agents should be provided in parks to facilitate hand washing. All cats and dogs who are at risk should be treated with anthelmintic agents, especially after giving birth. Because free-ranging and/or feral cats and dogs may be most at risk for contributing to this condition in the poorest neighborhoods, anthelmintic administration becomes a public health issue, requiring creative approaches (Hotez and Wilkins, 2009). Trap/neuter/release programs in cities with large numbers of cases of toxocariasis may wish to incorporate de-worming. The key to resolving all elimination concerns—even those involved in marking—is to recognize and be able to identify the pattern in the choices the cat makes about elimination. The pattern involved in the cat’s behavior tells us what the cat’s needs are. If clients can meet the cat’s needs, the problem will resolve. Otherwise, the biggest reason why cats are relinquished or euthanized involves elimination that the clients view as problematic. Clients will keep cats about whom they have complaints pertaining to elimination behaviors 2 years before relinquishing, abandoning, or euthanizing them. This is sufficient time to resolve even tough elimination problems, but problems can be resolved only if veterinarians screen every cat at each visit (Fig. 9-1). Specific diagnoses pertaining to lack of litterbox use and marking are individually discussed. An accompanying flow chart is provided in Figure 9-2. Fig. 9-2 Flow chart for treatment and diagnosis of feline elimination complaints. (Thanks to Mary Anna Labato, DVM, DACVIM, for input into a very early version of this flow chart.) Concerns about litterbox use generally involve one or more of the following client complaints: • The cat doesn’t use the box at all. • The cat uses the box for either urine or feces but not both. • The cat eliminates right next to or on the box but not in it. All of these could be normal behaviors, but when they represent a change in former behavior, they generally flag a behavioral problem. Ancestral cats, their wild relatives, and their feral counterparts may never cover their urine or feces. Not covering urine or feces may act to inhibit disease transmission if ova of parasites dry, but this behavior also acts to provide a visual and olfactory statement of feline presence and identity. In such cases, urine and feces are currency, not just elimination products. Some cats will never cover their urine and/or feces but may still vigorously scratch in the box. If the cat’s behavior changes and previously covered urine and/or feces is now not covered, clients should also be alert to changes in scratching behaviors. Cats who like their litterboxes scratch a lot, whether or not they cover urine and/or feces (Sung and Crowell-Davis, 2006). Complaints about litterbox use are almost always related to one of four diagnostic categories: • substrate preference for elimination, • substrate aversion for elimination, • location preference for elimination, and These four diagnostic categories are represented by the heuristic scheme in Table 9-1. • Non-spraying marking: The pattern of deposition of urine or feces distinguishes non-spraying marking behavior from substrate or location aversions/preferences. When non-spraying marking is a consideration, the amounts of urine or feces are small and distributed over areas associated with social stimuli, not with substrates or locations (Table 9-2). TABLE 9-2 Patterns That Separate Non-Spraying Marking from a Substrate or Location Preference or Aversion • Marking behavior involving spraying: In marking involving sprayed urine (spraying), the cat treads on its front feet, raises its tail, quivering the tip, and sprays urine vertically (Fig. 9-3). If the cat is not backed against a vertical surface, sprayed urine makes a linear pattern on horizontal surfaces. Urine sprayed against a vertical surface drips and puddles (Fig. 9-4). Regardless, sprayed urine covers a larger surface area with urine than does squatting and so likely communicates different information than urine voided in a squat. The information communicated could simply be that the cat was confident enough to engage in the very visual behaviors that accompany spraying. Both male and female cats can and will spray, as will neutered/desexed cats. Neutering can decrease or stop spraying if it has been occurring for only a short while or it is related solely to estrus cycles or responses to them, and neutered cats spray less frequently than do cats who have not been neutered. Fig. 9-3 Cat spraying against a bush. Notice the elevated, curled, and moving tail; the arched back; the movement of the ears; the stare; and the treading and movement of the hind legs. (Photo courtesy of Anne Marie Dossche.) Risk factors for aversions, preferences, and marking are found in Box 9-1. Diagnostic Criteria and Description: • Consistent elimination in an area or areas that are linked by some common sensory aspect. • Common sensory aspects may include: • open, smooth, reflective surfaces (e.g., tile floors, bathtubs, kitchen counters), • soft, silky substrates (e.g., some silicacious litters, pearlized litters, clothes, towels, bath mats, plastic trash bags), • soft, thick, absorptive surfaces (e.g., thick silk and wool rugs), • soils, sands (e.g., houseplants), and • soft, non-particulate, absorbent materials (e.g., paper towels, newspapers). • Cats who use their litterboxes consistently and who scratch and dig in them are using a preferred substrate. The clients agree that this substrate is one suitable for elimination. • Cats who may be identifying preferred non-litter substrates to clients may be exhibiting completely normal behavior, but clients find it offensive. The diagnosis is made only when there is a client-pet preference mismatch. • Cats who develop aversions to litter substrates or locations will usually develop a secondary preference for another substrate or location. • As substrate preferences become more narrow and restrictive, the greater the risk that truly abnormal behavior may be involved. • Clients find urine and/or feces on non-litter substrates. • When the clients can list every substrate ever used, these substrates are usually linked by some shared sensory—often tactile—characteristic. • Finding urine and/or feces on non-litter substrates may be preceded by changes in litter (clients changed brands) and/or litterbox hygiene (e.g., change in frequency and quality of cleaning). • Clients may not realize that the cat is eliminating elsewhere unless they monitor the litter for changes in use (e.g., changes in volume of urine/feces). • In the case of a substrate preference, cats may be seen scratching around but not in the litterbox. • Cats with substrate preferences may sniff and scratch a series of areas before beginning to eliminate on them, so clients should use these behaviors to watch for changes in litterbox use. • Cats with urinary tract infections (UTIs) may not be able to make it to the litterbox or be too painful to get into and out of the box as needed and may eliminate on any substrate available or near the litterbox. • Older and arthritic cats may develop new preferences if they are unable to get into and out of the litterbox without pain. • If the cat is eliminating in a pattern that does not seem to be associated with how something feels, or where the substrate is, and the social environment appears to contain minimal stressors, a medical problem may be involved. The most common medical conditions that are associated with complaints about elimination are feline lower urinary tract signs/disease (FLUTD), bacterial cystitis, urethral obstruction, diabetes mellitus, cognitive dysfunction (CD), hyperthyroidism, lower motor neuron disease, enteritis/colitis, parasitemia. • The standard database for inappropriate elimination involving urination includes a physical exam, complete blood count (CBC), serum biochemistry profile, urinalysis with culture, and thyroid profile (if the cat is >6 years old). For complaints involving defecation, a fecal flotation and direct smear should be included. Etiology, Epidemiology, and Risk Groups: • Substrate preferences for elimination are extremely common, particularly among long-haired cats. Long, soft hair may collect more odor and/or pieces of litter, and so cats may learn early to prefer a substrate that allows them to remain free of material and odor. • Histories for many affected cats may contain information about an extended period where the clients were ill, busy, or away and not changing the litter as often as before. • The “substrate preference” in this case may be as simple as clean litter. If the client reports that the cat gets into the box and enthusiastically uses it every time it is cleaned and changed, it is likely that the cat has a preference for very clean litter. • If the cat cannot escape filthy litter, he may start to sample other substrates and learn that he likes these as well or better than the litter he had previously been using. In such cases, a change in substrate type may be needed. • The illness of one cat in the household may alter the perception of the litter for the other cats and cause them to sample other substrates. If any cat in the household is taking medication or has hepatic, renal, or gastrointestinal illness, clients should be advised to provide additional litterboxes for the well cats and/or observe them to learn if the illness is a problem for them. • Cats who have been ill and either been forced to or had the experience of eliminating on a non-litter substrate can learn to prefer the new substrate. • Cats who have undergone any surgery, including onychectomy (declaw), may find traditional litters painful and learn to prefer things like fabric, plastic, paper, and smooth surfaces that cannot get caught in or abrade their wounds. This preference may persist after recovery. Common Myths That Can Get in the Way of Treatment or Diagnosis: • The common myth about elimination concerns is that the cat is doing this to “get even” with the client, for “spite” because the cat is “angry,” and/or as a way to show displeasure about some aspect of the client’s choices. • This is among the most anthropocentric of myths about cat behavior. If the client can be convinced to understand the cat’s needs, the client usually understands that the cat is being put in a situation that is uncomfortable or untenable. • Humans will seldom use filthy toilets unless there is no other option. Noting this may result in some understanding of the cat’s concerns. Commonly Asked Client Questions: • Will the cat return to using her litter if we clean more frequently? • Not necessarily. If this is a true preference, the litter offered will need to reflect the cat’s preference. • Can we switch the cat back to her original litter, gradually and over time? • Possibly, but the cat needs to be using an identified substrate 100% of the time for a prolonged period of time (weeks to months, depending on how long the problem had been ongoing before treatment) before this is even attempted. Once the clients are sure that the cat is eliminating in the litterbox using one substrate, the clients can gradually change the ratio of that substrate to the one they wish the cat to use. Very gradual changes over 1 or 2 months may provide the best outcome. • If there is an accompanying aversion to the old litter, switching the cat back to his or her old litter will not work. The extent to which a cat becomes averse may depend considerably on the cat. • Why does the cat seem to prefer the bathroom floor/hardwood floor/tile floor/bathtub/shower? • All of these surfaces share in common that they are reflective, cool, and well drained. This is the ancestral condition that cats sought for elimination. The cat may be making an innate choice, and that choice may be hard to shift. Mimic the substrate to the extent possible, up to and including lining a litterbox with tiles. These types of litterboxes can be washed, and if the tiles are not glued to the litterbox, they can go in the dishwasher. • If the cat is using the shower or tub and does not use a box placed in that area with a similar substrate available, it is going to be very hard to shift that preference, and the client may wish to settle for a situation that is at least easy to clean. • How do we know which cat is doing this? • Cats who potentially defecate on inappropriate substrates can be given colored wax—which is what most non-toxic crayons are—by grating it into their food. Clients can use different colors simultaneously for different cats if they can guarantee that each cat eats only his food. The wax passes through the cat’s gastrointestinal tract with the color intact. • Red beets also are detectable in feces and can be fed to cats (one cat at a time). • Fluorescein can be given to cats to learn who is responsible for the urination. A detailed explanation is found in the section on spraying. • Clients should try to identify the types of substrates that the cat uses and mimic those. • Clients should be encouraged to watch cats use litter. If the cat scratches and digs in the litter and gets into it to do so, the cat likes the litter. • Litterboxes also matter and may not be separate from the litter preference for cats. • Liners should not be used. They affect the way the cat detects the substrate and invariably are linked with decreased use of the litter by cats. • Because cats are so good at smelling and identifying odor, the clients must clean well and thoroughly any affected area. • If the problem involves a strong, innate preference, behavior modification is not likely to be successful. • If the cat has engaged in a sampling process after an illness, a vacation, or other inducements not to use the box without developing an aversion, and if the cat is social and will use the box in the client’s preference, the client may be able to reward the cat with praise and a treat for getting into and using the box. There are no data to suggest the extent to which this can help, but it cannot hurt. • Medication/dietary intervention: • If the cat has developed an aversion or a concern about any aspect of the litter or box, he or she may be difficult to convince to use a litter everyone can agree on without using an anti-anxiety medication. Medications that may help include: • Before using medication, a laboratory evaluation (CBC, serum biochemistry profile) and at least a lead II electrocardiogram (ECG), especially if considering TCA/SSRI use, should be performed. Most of these medications are metabolized through renal and hepatic pathways, and clearance may be altered if renal or hepatic disease is a concern. Additionally, these medications will interact with other medications that share the same cytochrome P-450 system enzyme pathways, so a good medical history is important. TCAs and SSRIs may be more arrhythmogenic in cats than in other species. • Cats older than 6 years should also have a thyroid profile as part of their baseline laboratory evaluation. • Cats treated with monoamine oxidase (MAO) inhibitors (some flea and tick collars) should not be treated with TCAs or SSRIs. • Medication use will need to continue for at least a few months until the clients are certain that the cat is always using the litter and is not distressed. • Withdrawal should be gradual (see the “Protocol for Using Behavioral Medication Successfully”). • Full withdrawal of medication may not be possible for all cats. • If the cat is painful, the aversion may be related to the pain. Treatment of pain is essential for the cat’s quality of life (QoL).
Undesirable, Problematic, and Abnormal Feline Behavior and Behavioral Pathologies
Overview of Feline Behavioral Concerns
Zoonotic Concerns Relevant to Patterns of Feline Behavior
Cat-Scratch Disease
Toxoplasmosis
Toxocariasis
Feline Behavioral Concerns Involving Placement of Urine/Feces as Part of Inappropriate or Undesirable Elimination Behavior
Cats Who Do Not Use Their Litterbox
Covering Urine and Feces
Feline Marking Behaviors Using Urine or Feces

Diagnostic Categories for Elimination Complaints
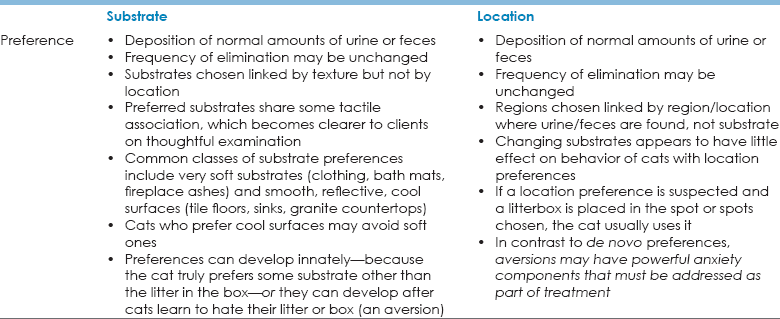
Substrate Preference for Elimination
 Some silicacious, clumpable litters are extremely soft and may be palatable to cats who like soft substrates.
Some silicacious, clumpable litters are extremely soft and may be palatable to cats who like soft substrates.
 Litterboxes can be tiled or covered in impermeable surfaces that cats like.
Litterboxes can be tiled or covered in impermeable surfaces that cats like.
 Empty litterboxes or a cookie tray may be used by cats who prefer flooring.
Empty litterboxes or a cookie tray may be used by cats who prefer flooring.
 If the cat likes a very soft, trackable litter, clients can put the box on a mat that attracts dust and litter to limit tracking.
If the cat likes a very soft, trackable litter, clients can put the box on a mat that attracts dust and litter to limit tracking.
 Litterbox condition matters. Deeply scored boxes feel rough and hold odor. Boxes should be well washed, rinsed, and dried as needed but at least once a week.
Litterbox condition matters. Deeply scored boxes feel rough and hold odor. Boxes should be well washed, rinsed, and dried as needed but at least once a week.
 Any residual bleach smell may deter use because bleach kills olfactory neurons, which alters the cat’s ability to assay his or her sensory environment.
Any residual bleach smell may deter use because bleach kills olfactory neurons, which alters the cat’s ability to assay his or her sensory environment.
 Linear dimensions of boxes matter.
Linear dimensions of boxes matter.
 Arthritic cats and young kittens may be unable to get into tall boxes and so will not use them.
Arthritic cats and young kittens may be unable to get into tall boxes and so will not use them.
 If the litterbox is at least 1.5 times the body length of the cat, the cat is much more likely to use it (Sung et al., 2006).
If the litterbox is at least 1.5 times the body length of the cat, the cat is much more likely to use it (Sung et al., 2006).
 If one cat is using the box, the clients may be able to go 2 to 3 days without completely emptying the litterbox if the litter is scooped multiple times a day.
If one cat is using the box, the clients may be able to go 2 to 3 days without completely emptying the litterbox if the litter is scooped multiple times a day.
 If multiple cats are using any box, the box will need to be completely emptied daily.
If multiple cats are using any box, the box will need to be completely emptied daily.
 This recommendation is predicated on having a small household of cats. What is “small” depends on how the cats get along, whether the cat group contains any family members, the size of the dwelling, the health of the cats, and the number of floors available to the cats.
This recommendation is predicated on having a small household of cats. What is “small” depends on how the cats get along, whether the cat group contains any family members, the size of the dwelling, the health of the cats, and the number of floors available to the cats.
 Litterboxes should be arranged in a way that allows clients to learn what the cat needs and wants.
Litterboxes should be arranged in a way that allows clients to learn what the cat needs and wants.
 Clients may like litterboxes with lids, but cats generally may not.
Clients may like litterboxes with lids, but cats generally may not.
 Individual cats may have individual preferences with respect to type of box (Grigg et al., 2013), despite no reported statistically significant group preferences for cats offered open vs. covered litter boxes in a small study.
Individual cats may have individual preferences with respect to type of box (Grigg et al., 2013), despite no reported statistically significant group preferences for cats offered open vs. covered litter boxes in a small study.
 Enclosed boxes concentrate odor and ammonia vapor.
Enclosed boxes concentrate odor and ammonia vapor.
 Tramadol, a synthetic opioid that stimulates mu receptors, also affects serotonin receptors and may provide some very mild anti-anxiety effects. If tramadol is given with TCAs or SSRIs, clients should be advised that there is a very small risk of serotonin syndrome. If the client is taught how to monitor the cat, the risks are minimal.
Tramadol, a synthetic opioid that stimulates mu receptors, also affects serotonin receptors and may provide some very mild anti-anxiety effects. If tramadol is given with TCAs or SSRIs, clients should be advised that there is a very small risk of serotonin syndrome. If the client is taught how to monitor the cat, the risks are minimal.![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree