Chapter 18 Tracheostomy
• Continuous patient monitoring and intensive nursing care are critical to successful tracheostomy tube management and patient comfort.
• Care must be taken to prevent damage to the left recurrent laryngeal nerve when a tracheotomy is performed.
SURGICAL TECHNIQUE
Transverse Incision
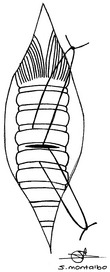
The annular ligament between the third and fourth or fourth and fifth tracheal rings is incised, taking care not to extend the incision longer than 50% of the tracheal circumference. Extreme care must be taken to avoid the left recurrent laryngeal nerve. A small ellipse of cartilage from each tracheal cartilage adjacent to the tracheotomy incision can be made to help reduce tracheal irritation and inflammation. Long loops of suture are placed around the tracheal rings adjacent to the incision to facilitate retraction of the trachea and future replacement of the tube after cleaning (Figure 18-1).1,2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


