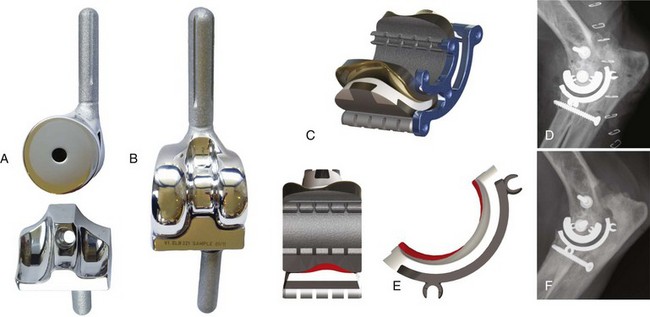
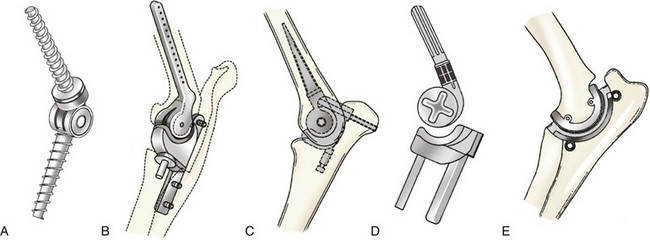
Chapter 54 During the past two decades, functional limitations of conservative management and nonreplacement surgeries for the treatment of end-stage canine elbow osteoarthritis have fueled growing interest in total elbow replacement. Clinical use of a total elbow replacement was first reported by Whittick, who in 1964 used a custom-made spherical hinged prosthesis to treat a gunshot-induced comminuted elbow fracture in a cat.17 To our knowledge, the first clinical canine total elbow replacement was implanted in 1989 by Chancrin, who used a prototype cemented hinged prosthesis to treat a Labrador Retriever afflicted with end-stage osteoarthritis and severe ankylosis (Figure 54-1, A).5 Subsequently, in 1996, Lewis reported on the first clinical results of a hinged total elbow replacement implanted in 10 dogs.15 In these first-generation systems, Chancrin and Lewis used cemented, fully constrained hinged designs (linked systems). Because of the rigid mechanical link between the humeral and radioulnar (RU) components, most of the forces across the joint were transmitted through the implant to the cement and its interfaces.4 The high complication rates encountered with these initial designs quickly led to a paradigm shift to unlinked total elbow replacement designs (Figure 54-1, B through E). Vasseur,16 Lewis (second and third generations),15 Cook,12 and Conzemius6,10 developed the first unlinked designs in the late 90s (Figure 54-1, B and C). All encountered unacceptable postoperative morbidity that led to termination or further refinement of the respective designs. Following iterations of his earlier designs (Figure 54-1, D), Conzemius reported encouraging results after total elbow replacement in 6 normal dogs, then 2 years later in 20 dogs afflicted with naturally occurring osteoarthritis.7,8 Minor modifications, including the addition of porous coated surfaces to the lateral and medial aspects of the humeral component, as well as a curvilinear humeral articular profile, led to Conzemius’ fifth total elbow replacement generation, which became commercially available in 2005 (Iowa State system, BioMedtrix, Boonton, NJ). Recently, a radically novel total elbow replacement design (TATE Elbow system, BioMedtrix) was developed by Acker and Van Der Meulen (Figure 54-1, E).2,3 Similar to Conzemius’ prosthesis, the TATE uses an unlinked, semiconstrained design. However, several fundamental differences exist between these two systems. Unlike previous conventional stemmed and cemented prostheses, the cementless TATE implant was designed to use a novel resurfacing concept, as well as less invasive surgical approaches. In 2008, Acker and Van Der Meulen reported satisfactory results 6 months after implantation of this resurfacing prostheses in 6 dogs affected with end-stage osteoarthritis.1 Both currently commercially available prostheses (i.e., fifth-generation Iowa State and the recently released second-generation TATE Elbow systems) use unlinked semi-constrained two-component designs. In the absence of a rigid mechanical link between the humeral and radioulnar components, the stability of unlinked prostheses is provided by the matching geometry of the prosthetic articulating surfaces and the surrounding soft tissue envelope.4 Specifically, current total elbow replacement systems are designed so that some of the transarticular forces (e.g., the forces in varus-valgus) are almost exclusively counteracted by passive soft tissue constraints (i.e., collateral ligaments), while other forces (e.g., internal/external rotation and mediolateral translation) are also controlled by the geometry of the prosthetic articular surfaces. Although contributing to joint stability, prosthetic constraint has been shown to influence stresses at the bone-implant interface. Interfacial stress distribution is further complicated by the fact that both systems feature a single radioulnar component that eliminates motion between the radius and the ulna. Although the ideal prosthesis should allow near-normal joint kinematics of humeroantebrachial and radioulnar joints, such a design would likely require more complex three-component prostheses. The current designs were likely chosen as a compromise between optimal joint kinematics and decreased prosthetic complexity and related risk of implant failure. Design modifications have been recently devised for both systems in response to their respective (documented or potential) shortcomings. In an attempt to reduce the rate of post-operative elbow luxation, Conzemius’ team is currently developing a highly constrained, metal on metal, total elbow replacement system Figure 54-2, A and B.15a Although this new design has been shown to offer greater intrinsic stability than the fifth generation Iowa system, to the author’s knowledge, this system has not been used in live dogs. Similarly, in an effort to optimize bone ingrowth a second generation TATE Elbow system was released early 2010 (Figure 54-2, C and E). This refined design has been used in ~30 clinical cases worldwide (Figure 54-2, D and F). Design modifications included hollow primary fixation posts and hydroxyapatite coating. In addition, reduced prosthetic constraint in rotation and mediolateral translation was achieved through modification of the radioulnar articular profile.13b,13c Although no cases of implant loosening had been observed with either TATE generation, these design iterations, were mainly intended to promote implant osteointegration. Figure 54-2 Photographs of the newest total elbow replacement prosthesis designed by Conzemius’ group (A and B). This new design is a highly constrained, metal-on-metal, hybrid fixation system. While the humeral stem is cemented, stability of the radioulnar (RU) component relies on a dual fixation mechanism. Primary fixation is provided by an ulnar screw through the RU median ridge, while long-term stability relies on osteointegration of the radial peg. Humeral and RU components are highly congruent. The humeral component features a prominent medial section, a deepened median trochlea, and a smaller capitulum. Schematic of a second generation TATE cartridge (C). This new design features hollow humeral and radioulnar posts, hydroxyapatite coating, and a modified articular profile. Front view of a TATE cartridge (E, left) and side view of the radioulnar component (E, right) illustrating the modification of the cranial and caudal aspects of the RU polyethylene profile (red areas) between first and second generations. The median RU ridge was flattened in the second generation TATE to reduce prosthetic constraint. Immediate (D) and 12 month (F) postoperative mediolateral radiographs after implantation of a second generation TATE. This patient had received a first generation TATE on the contralateral elbow 21 months earlier (see Figure 54-4). Note the absence of radiolucent line at the bone-implant interfaces. (Photographs from Reunan P. Guillou, CAD drawings by Greg Van Der Muelen, radiographs from Loïc M. Déjardin.) The primary indication for total elbow replacement is severe, intractable degenerative joint disease that is not responsive or is poorly responsive to medical management. Although elbow osteoarthritis is most commonly associated with elbow dysplasia, it can also result from articular fracture, elbow luxation, or angular limb deformities with subsequent elbow incongruity. Because of the potential complications and/or limited long-term follow-up available for the currently available systems, total elbow replacement should be restricted to older dogs with a clearly decreased quality of life on a day-to-day basis, which cannot be satisfactorily managed with medical treatment. As for any total joint replacement, systemic or local infection (e.g., local pyoderma, bacterial cystitis, otitis externa, periodontal disease) increases the risk of postoperative infection and should be identified and addressed before surgery. Chronic elbow luxation is a relative contraindication to total elbow replacement. The compromised periarticular soft tissue envelope may indeed increase the risk of postoperative luxation with the currently available, unlinked systems. Successful use of the Iowa State system after chronic elbow luxation has been reported.7 Finally, severe malunion may preclude the use of the resurfacing TATE Elbow system. Such cases may be successfully addressed using the Iowa State system.7 Neurologic dysfunction and skeletally immature dogs represent other potential contraindications.
Total Elbow Replacement in Dogs
Current Systems—Design Rationale and Evolution
Indications/Contraindications
< div class='tao-gold-member'>
Total Elbow Replacement in Dogs
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


