12 The polydipsic cancer patient
INTRODUCTION
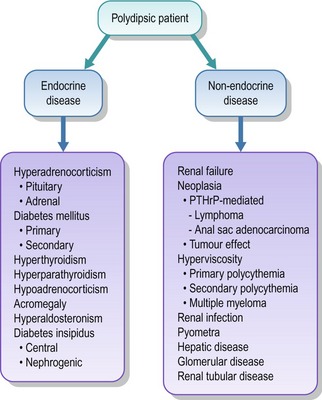
Polydipsia is defined as when an animal drinks in excess of 100 ml/kg/day, although a high degree of suspicion for polydipsia can be reached when daily water intake exceeds 80 ml/kg. Interestingly, many owners are much more aware of the polyuric aspect of polydipsic patients, which is probably not surprising, especially if the patient is incontinent. Because investigation of polydipsic patients encompasses many possible different medical and oncological conditions, it is vital that a logical and step-wise approach is taken with such patients. Very broadly, polydipsic patients can be grouped in many different ways but the flow diagram in Figure 12.1 gives one possible framework to investigate polydipsic patients along with the major differential diagnoses for each group.
CLINICAL CASE EXAMPLE 12.1 – MEDIASTINAL LYMPHOMA IN A DOG
Presenting signs
Excessive drinking (approximately 120 ml/kg/day), dullness, lethargy and inappetance.
Case history
The relevant history in this case was:
Clinical examination
Diagnostic evaluation
Treatment
Whilst waiting for the laboratory results, the dog was hospitalized and received intravenous fluid therapy at four times maintenance (i.e. 8 ml/kg/hour) in an attempt to help reduce his hypercalcaemia. Once the diagnosis was confirmed, the owner agreed to commence chemotherapy, as the optimal treatment for mediastinal lymphoma remains systemic chemotherapy in most cases. A Madison-Wisconsin protocol was used for this dog, as detailed in Appendix 2.
Theory refresher
Lymphoma is one of the more common tumours seen in dogs, estimated to account for between 7 and 24% of all reported canine tumours. It is most commonly seen in middle-aged to older dogs and there appears to be no gender predisposition for the disease. Lymphoma and lymphosarcoma are interchangeable terms, although as lymphatic tissue is technically mesenchymal in origin, the term lymphosarcoma is technically more correct. The neoplastic cells develop from a clonal expansion of lymphocytes located in any of the sites within which lymphoid cells may be found. As a result, there are many different forms of the disease and currently several different classification systems, which can make interpretation of pathology reports difficult! However, in practical terms, the classification systems do not really change the initial clinical approach to the disease, which is to:
The clinical usefulness of cytology can be enhanced by having flow cytometry undertaken at the same time. Flow cytometry is a technique in which cells are sorted according to their size and then investigated to see what external molecular markers they carry by using monoclonal antibodies that bind to cell surface molecules. Flow cytometry can be extremely useful in the diagnosis of lymphoproliferative diseases, as there are some markers such as CD45, that clearly label a cell as being a leucocyte. There are markers that are unique to B lymphocytes (e.g. CB21 and CD79a) or T lymphocytes (e.g. CD3, CD4, CD8) and markers that are only found on immature cells (e.g. CD34), thereby identifying the cell as being a blast. By using this specific identification technique, cells can be accurately identified; both by their specific family subtype but also by their stage of maturity and therefore are determined as neoplastic or normal. Flow cytometry has been shown to be especially helpful in the differentiation between thymoma and lymphoma, which cytologically can be a challenge as the thymus contains lymphoid cells in various stages of maturation as a natural physiological feature (see Fig. 8.8). Thymomas can also cause a dog to become hypercalcaemic in a minority of cases (up to 30% in one series), so the identification of hypercalcaemia in a patient with a mediastinal mass does not rule out a diagnosis of thymoma. It has been shown that thymomas in dogs can be identified by undertaking flow cytometry on cells obtained by ultrasound-guided aspirates of mediastinal masses and identifying more than 10% of the cells as having both CD4 and CD8 staining, whereas lymphoma cases stained for these markers on less than 2% of cells. This is why this technique was performed in this clinical case example.
If histopathology is undertaken, the classification system in Box 12.1 is the one most frequently referred to in the UK.
Box 12.1 World Health Organization Clinical Staging System for Lymphosarcoma in Domestic Animals
Stage
What the various classification systems have been useful to show is that:
Hypercalcaemia is more commonly associated with T-cell lymphoma (although it does develop in B-cell patients) and the identification of hypercalcaemia used to be thought of as a negative prognostic indicator. However, it is now clear that it is the B- or T-cell delineation that has the negative prognostic indications rather than the hypercalcaemia per se. The hypercalcaemia is induced by the production of parathyroid-hormone-related peptide (PTHrP) by the neoplastic cells, as documented in the case presented. PTHrP is elevated in many tumours (with the subsequent development of hypercalcaemia) but it is most commonly associated with lymphoma, anal sac adenocarcinoma and multiple myeloma. The other main differential diagnoses for hypercalcaemia in the dog and cat are given in Box 12.2.
Prognosis
The choice of treatment protocol for the multicentric form of lymphoma may also affect the prognosis in some cases. It has been shown that dogs treated with a doxorubicin-containing protocol in general have a reduced risk of relapse and death when compared to dogs treated with a non-doxorubicin-containing protocol. Furthermore, multidrug protocols generally result in longer remission times and greater survival figures when compared to single-agent treatments. Pretreatment with steroids should be avoided if at all possible, as steroids appear to increase the risk of multidrug resistance gene expression, leading to reduced success rates with other chemotherapeutic agents. However, many factors need to be considered when choosing the correct protocol for each case, such as treatment cost, treatment frequency and duration, the suitability of the patient for injectable treatments and the risk of toxic side effects, to name but a few. Therefore, a summary of the most commonly used treatment choices is given below:



