Chapter 28
The Adrenal Gland
The increased availability and use of modern imaging techniques such as ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) have resulted in increased detection of adrenal masses and adrenomegaly. While some of these lesions may be incidental findings, some cases may require a definitive diagnosis, and cytology may be a valuable tool for initial evaluation. However, caution should be taken when considering adrenal fine-needle aspiration (FNA), especially in canine patients, as aspiration of pheochromocytomas may result in significant patient morbidity or possibly mortality from hypertensive or hypotensive emergencies and cardiac arrhythmias.1
Normal Cellular Components
The adrenal glands are composed of two parts: (1) the cortex and (2) the medulla. The cortex is derived from the mesoderm and is divided into three zones functionally and histologically. Adjacent to the capsule is the zona glomerulosa, followed by the zona fasciculata and the zona reticularis, which is closest to the medulla. The cells in the zona glomerulosa (Figure 28-1) produce and secrete aldosterone and are arranged in irregular columns histologically.2 The middle zone, the zona fasciculata (see Figure 28-1), is the thickest layer of the cortex and functions with the thinner inner layer, the zona reticularis, to produce cortisol and androgens respectively.2 Histologically, these two layers may be difficult to differentiate.
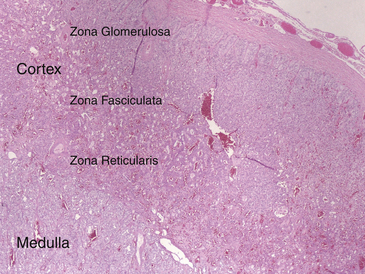
Figure 28-1 In this histologic section of normal canine adrenal gland, the cortex and medulla may be differentiated and the layers of the cortex may be observed. (H&E stain. Original magnification 100×.)
In the human medical literature, the cells from the zona fasciculata and glomerulosa appear similar cytologically and are oval to polygonal with abundant, foamy to vacuolated cytoplasm because of intracytoplasmic lipids; cytologic descriptions in dogs and cats are similar.3,4 Cells from the zona reticularis are lipid poor, containing eosinophilic granular cytoplasm with no vacuoles, but some cells from this zone may contain lipofuscin granules.3,4 The medulla, derived from neuroectoderm, secretes catecholamines. Cytologically, these cells appear different from adrenocortical cells and are sometimes described as resembling small-sized hepatocytes, with centrally to eccentrically located nuclei and finely granular cytoplasm.4
Abnormalities of the Adrenal Gland
Nonneoplastic Conditions
Adrenalitis
Primary adrenalitis is uncommonly reported in the literature, but when observed, canine and feline adrenalitis is often seen with septicemia or disseminated disease. Adrenalitis may occur with bacterial septicemia; disseminated fungal infections such as Coccidioides immitus, Histoplasma capsulatum, and Cryptococcus neoformans; and some protozoal infections such as Toxoplasma gondii and Babesia spp.4 Granulomatous inflammation may be seen with fungal organisms, whereas some protozoal infections elicit mild histiocytic infiltration and necrosis.4,5 Depending on the inciting cause, edema and hemorrhage may also cause adrenomegaly with systemic infections.5
Adrenocortical Hyperplasia
Adrenocortical nodular hyperplasia is most common in older cats and dogs. Diffuse cortical hyperplasia may also result in adrenomegaly, typically caused by oversecretion of adrenocorticotrophic hormone (ACTH) by a pituitary neoplasm.2 Histologically, hyperplasia of the adrenal cortex results in increased width of the cortex, often because of multiple nodules of hyperplasia, consisting primarily of the zona reticularis and the zona fasciculata (Figure 28-2).2,5 Fine-needle aspirates of these areas contain cells resembling those described from the normal zona fasciculata. Cytologic preparations are often cellular, and cells may be more tightly arranged than typical adrenocortical cells. Binucleate cells are commonly reported in aspirates from human adrenocortical hyperplasia.3 Differentiation of adrenocortical nodular hyperplasia from well-differentiated adrenal neoplasms may be challenging cytologically and will be further discussed in the next section.
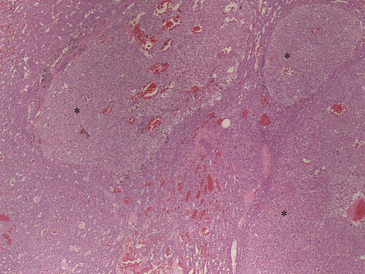
Figure 28-2 Histopathology of a canine nodular adrenal gland reveals three nonencapsulated, poorly demarcated nodules of cortical cells (∗) that have slightly different staining characteristics relative to the adjacent normal cells (adrenocortical nodular hyperplasia). (H&E stain. Original magnification 100×.)
Primary Tumors of the Adrenal Cortex
Functional adrenal cortical neoplasms are reported to be the underlying cause of approximately 10% to 15% cases of canine hyperadrenocorticism.4 Rare cases of feline hyperaldosteronism are associated with adrenal neoplasms.6,7 Neither cytology nor histopathology can determine whether a tumor is functional and serum adrenal function tests are necessary.
FNA cytology of adrenal nodules cannot be used to assess encapsulation or invasiveness, which may make cytology a difficult tool for definitive classification of adrenocortical nodules.3 Even histologic classification of adrenal lesions, including differentiation of normal from hyperplastic tissue, hyperplastic nodules from adenomas, and in some cases differentiation of adenomas from carcinomas, may be challenging. Distinguishing adrenocortical carcinomas from pheochromocytomas may also be problematic in some cases.2 In general, with increased malignancy of adrenocortical neoplasms, decreased lipid and increased nuclear atypia are encountered.3 Necrosis is reportedly a common feature in human adrenal tumors.3 Overlapping features of benign versus malignant adrenocortical nodules exist; however, cellular features at opposite ends of the spectrum, for example, benign adrenal cortical nodules may often be differentiated from a poorly differentiated adrenal cortical carcinoma.3 Regardless, limitations of cytology should be recognized and cytologic findings should be used in conjunction with the patient history, clinical signs, blood work abnormalities, and imaging, if available.
Adrenocortical Adenomas and Carcinomas
Adrenal adenomas are common in older dogs and found only rarely in cats.2 Histologically, adrenal adenomas are surrounded by a capsule and compress adjacent normal cortex (see Figure 28-3). Cells within adrenocortical adenomas resemble the zona fasciculata or reticularis.4 Cytologically, adenomas are composed of cells similar to the normal zona fasciculata or reticularis and are round to polygonal, often containing several discrete vacuoles within moderate to abundant amounts of eosinophilic cytoplasm (Figure 28-4). Nuclei are typically round, and indistinct nucleoli are occasionally observed. Cells may exhibit mild anisocytosis and anisokaryosis.5 In humans, adrenal adenomas may sometimes exhibit more cellular pleomorphism.3 Some adenomas will also contain extramedullary hematopoiesis (Figure 28-5).8
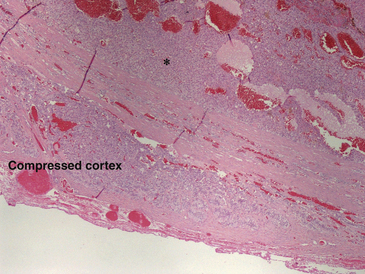
Figure 28-3 Histopathology of a canine adrenocortical adenoma reveals an expansile, densely cellular, encapsulated mass (∗) compressing normal cortex (labeled). Cells are arranged in packets supported by thin wisps of fibrovascular stroma. On higher power, individual cells were large, polygonal, with prominently vacuolated eosinophilic cytoplasm and clearly defined cellular borders. (H&E stain. Original magnification 100×.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


