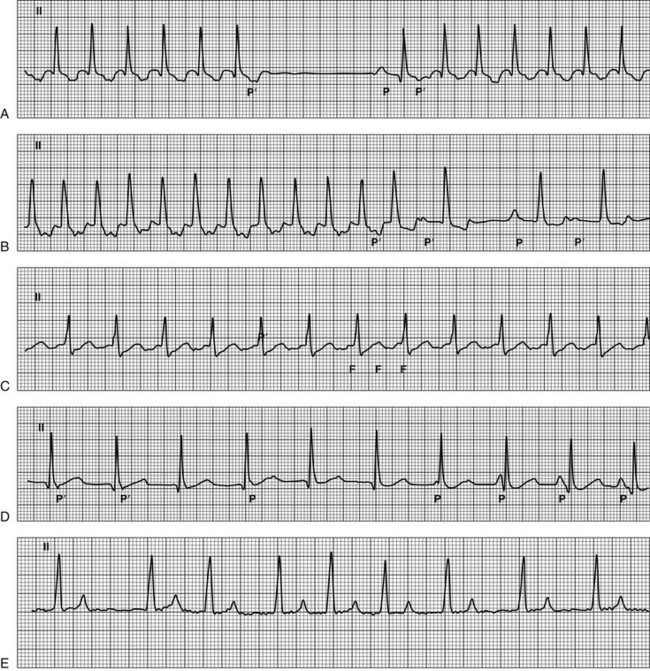
Chapter 171 Tachyarrhythmias are rapid rhythms, with rates typically above 180 to 200 beats/min in dogs, that appear out of proportion to the animal’s level of activity or stress. This chapter outlines the diagnostic approach and management strategies for common and uncommon supraventricular tachyarrhythmias (SVTs) in dogs. Additional information regarding management of focal atrial tachycardias, atrial flutter, and atrial fibrillation can be found in Chapters 175, 176, and 178. In the last decade, detailed endocardial mapping has established the underlying arrhythmogenic mechanism and the site of origin of the most common SVTs in the dog. With this information as a guide, a stepwise approach to ECG interpretation can be used to diagnose SVTs (Figure 171-1). The duration of the QRS complex is the first parameter that should be assessed to distinguish SVTs from ventricular tachycardia. This step should be followed by determination of the ventricular rate, the regularity of the R-R interval, signs of atrial activation, the relationship between ventricular and atrial activation, presence of QRS complex alternans, ST-segment anomalies, and finally the AV conduction ratio during tachycardia. Signs of ventricular preexcitation, characterized by a consistent and short P-R interval, should be sought during periods of sinus rhythm. Figure 171-1 Surface electrocardiographic tracings of common supraventricular tachyarrhythmias. A, Orthodromic atrioventricular reciprocating tachycardia. The first part of the tracing shows a narrow-QRS tachycardia with a regular cycle length of 200 msec (300 beats/min); after the sixth beat the tachycardia stops suddenly and a sinus beat occurs (P); the tachycardia then restarts with the same cycle length. During the tachycardia a retrograde atrial activation is visible in the ST segment with an inferior-to-superior axis on the frontal plane (P′) and a short RP′ interval (shorter than 50% of the relative RR interval, RP′:P′R = 0.57). The P′R interval after the sinus beats is longer; this indicates prolonged conduction along the AV node, which triggers the onset of tachycardia. B, Focal atrial tachycardia arising from the crista terminalis. The first part of the tracing shows a narrow-QRS-complex tachycardia with a regular cycle length of 200 msec (300 beats/min). After the twelfth beat a cycle-length irregularity occurs characterized by a longer RR interval in which the ectopic atrial activation (P′) appears after the T wave; then a sinus beat occurs (P), followed by an ectopic beat. In the first part of the tracing, the P′ is superimposed on the previous ST segment with a superior-to-inferior axis on the frontal plane and a RP′:P′R of 0.8. After the twelfth beat, the depolarization rate of the ectopic focus decreases, which causes a longer RP′; AV conduction prolongation explains the longer P′R interval. C, Typical atrial flutter with a 2 : 1 conduction ratio. The tracing shows a narrow-QRS tachycardia with a regular cycle length of 240 msec (250 beats/min). Atrial activations (F) are continuous and regular with a saw-toothed appearance. Every other F wave is blocked in the AV node. D, Focal junctional tachycardia with 1 : 1 ventriculoatrial retrograde conduction progressing to isorhythmic atrioventricular dissociation. The first part of the tracing shows a narrow-QRS-complex tachycardia with a regular cycle length of 400 msec (150 beats/min). In all but the last beat the ventricular depolarization starts from the junctional area. The atria are depolarized in the first two beats in a retrograde manner along the AV node and appear as pseudo S waves (P′); then, starting from the third beat, the atria are depolarized by the sinus node at a progressively faster rate, which induces a shift of the P waves from the right to the left of the relative QRS complex with a secondary increase in the PQ interval (isorhythmic atrioventricular dissociation). As soon as the sinus rate is faster than the junctional rate, the ventricles are depolarized starting from the sinus node, and a sinus beat appears (last QRS complex). E, Atrial fibrillation. The tracing shows a narrow-QRS-complex tachycardia with an irregular cycle length and an average ventricular rate of 140 beats/min. Atrial activations are characterized by low voltage and oscillations of variable morphology (f waves). Lead II; paper speed, 50 mm/sec; calibration, 10 mm/mV.
Supraventricular Tachyarrhythmias in Dogs
Definition
Electrocardiographic Differential Diagnosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


