CHAPTER 6 Subcutaneous Glandular Tissue: Mammary, Salivary, Thyroid, and Parathyroid
Mammary gland lesions present special challenges due to the diversity of cell types that may be involved and the oftentimes overlapping cell populations within hyperplastic, dysplastic, benign, and malignant lesions. Reported diagnostic accuracy for cytologic differentiation of benign from malignant mammary neoplasms in dogs varies from 33% to 79%.1–3 A cytologic grading system for differentiation of benign from malignant mammary tumors in dogs based on 10 important criteria of malignancy has been proposed.1 In that study, the predictive value of a positive result was higher (90% to 100%) than that of a negative result (59% to 75%), suggesting that cytologic evaluation tends to underdiagnose mammary gland malignancies. Wet fixation and a Papanicolaou-type stain were used in that study, which are less frequently used by most cytologists, and were thought to allow better appreciation of some criteria of malignancy.
THE MAMMARY GLANDS
Normal Cytologic Appearance
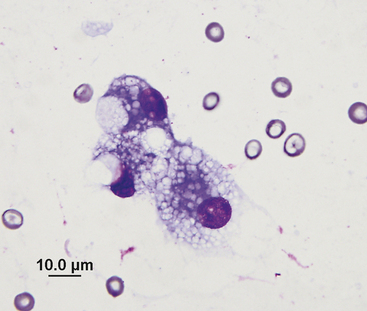
Mammary tissue of dogs and cats consists of five pairs of modified sweat glands that extend along the ventral body wall from the cranial thorax to the inguinal region. Glands consist of secretory acini and a series of excretory ducts. Myoepithelial cells lie between glandular epithelial cells and the basement membrane. During lactation the glands undergo marked hypertrophy to produce colostrum and then milk. Normal mammary secretions contain large amounts of protein and lipid droplets, and are of low cellularity. The predominant cell type in milk is the foam cell, a large, vacuolated epithelial cell that resembles an active macrophage (Figure 6-1). These cells usually occur singly. Small numbers of lymphocytes and neutrophils may also be present.
Benign Lesions
Mastitis
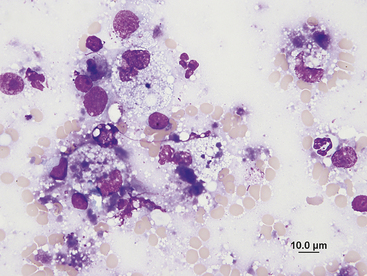
Mastitis, or inflammation of the mammary glands, may occur either as a diffuse form involving two or more mammae or as a focal lesion. Mastitis is usually associated with postpartum lactation or pseudopregnancy, and may result from ascending or hematogenous infections.4 Mammary secretions are usually adequate for diagnosis in cases of diffuse inflammation, whereas aspirates may be required for diagnosis of focal lesions. Smears are very cellular and contain large amounts of debris. Inflammatory cells may include neutrophils, lymphocytes, and macrophages in variable numbers, depending on the causative agent (Figure 6-2). Bacteria may be seen within phagocytes. Offending agents are usually coliforms, Streptococcus or Staphylococcus spp, although other bacteria and fungi may occasionally be isolated.5 Nonseptic mastitis, usually affecting the most caudal pair of glands, may occur secondary to milk stasis. Inflammatory cells will be present in variable numbers without accompanying bacteria.5 Focal, nonseptic inflammatory nodules may occur secondary to lobular hyperplasia. These are characterized by epithelial metaplasia, pigment-laden macrophages, nondegenerate neutrophils, lymphocytes, and plasma cells.6
Cysts
Mammary cysts result from a dysplastic process in which dilated ducts expand to form large cavitations.6 Cyst linings may consist of single layers of flattened epithelium or may have papillary overgrowth. Cysts may be present as single nodules or multinodular masses that grow slowly and have a bluish surface. Cysts are common in middle-aged and older bitches, but may occasionally appear in young dogs. Fluid aspirated is usually yellow, brown, green, or blood-tinged and of low cellularity unless there is concurrent inflammation. Cells are primarily vacuolated or pigment-laden macrophages. Epithelial cells aspirated from cysts lined by papillary projections may occur in dense clusters and exhibit a minor degree of nuclear pleomorphism.6 Because mammary cysts may be present along with benign or malignant neoplasia, sampling of solid tissue in addition to cystic fluid is recommended.
Solid Masses
Dysplastic lesions and benign epithelial neoplasms of mammary tissue include lobular hyperplasia, adenosis, adenomas, and papillomas, all of which contain similar cell populations.6,7 Smears made from aspirates contain many epithelial cells occurring singly or arranged in sheets and clusters. These cells generally exhibit little pleomorphism, having evenly dispersed chromatin and small, round nucleoli. However, dilated ducts can contain exfoliated epithelial cells that may have more criteria of malignancy than the rest of the mass.8 Sampling those cells for cytologic evaluation may result in a false impression of malignancy. Pigment-laden macrophages may be present (Figure 6-3). Some of these processes can also involve myoepithelial cells and connective tissue, further complicating the cytologic picture.7 Benign tumors involving stromal and epithelial elements, such as complex adenomas, fibroadenomas and benign mixed tumors, are common in dogs and sometimes seen in cats.6,7 Smears of aspirates from these lesions contain spindle shaped cells of myoepithelial or connective tissue origin in addition to clusters of epithelial cells similar to those described previously (Figure 6-4). These lesions can be difficult to differentiate even with histopathology due to the spectrum of cell types involved. Benign mixed tumors may produce cartilage, bone, or fat, in addition to fibrous tissue and epithelial tissue.7 Aspirates from these lesions may contain all these elements, but if a single population predominates the cytology can be misleading.9 Additionally, individual cell pleomorphism is occasionally marked in tumors considered benign due to lack of tissue invasion (Figures 6-5 and 6-6). Spindled mesenchymal cells are not a definitive cytologic characteristic of complex or mixed tumors, because they may also be found in some simple tumors.1
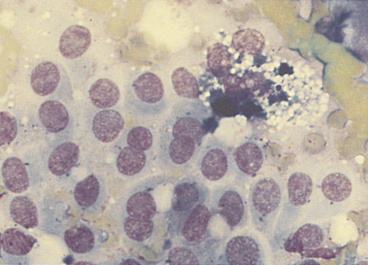
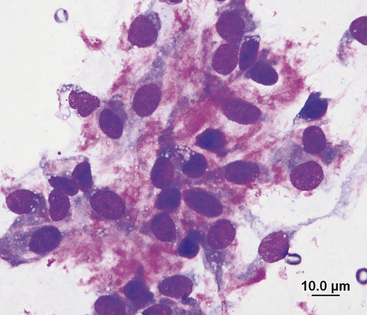
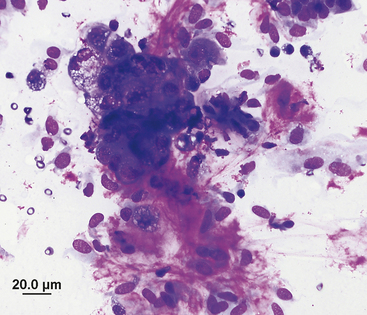
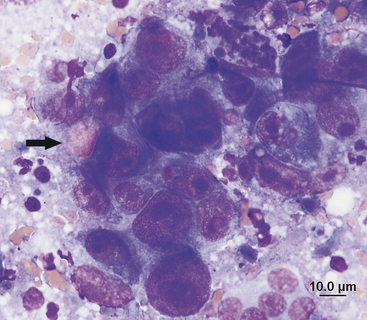
Figure 6-5 Canine mammary complex adenoma, same aspirate as Figure 6-4. Abundant eosinophilic matrix material and spindled mesenchymal cells near a cluster of vacuolated mammary epithelial cells. Epithelial cells exhibit moderate criteria of malignancy. (Wright’s stain, 500×.)
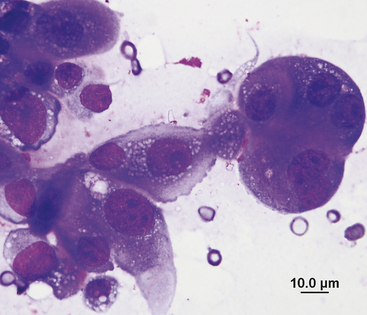
Figure 6-6 Canine mammary complex adenoma, same aspirate as Figure 6-4. These epithelial cells exhibit moderate to marked criteria of malignancy, including anisocytosis, anisokaryosis, and multiple prominent nucleoli. Histopathologic examination revealed this tumor to be well encapsulated and benign, despite individual cell pleomorphism. (Wright’s stain, 1000×.)
A specific form of mammary hyperplasia termed fibroepithelial hyperplasia/hypertrophy or fibroadenomatous change has been recognized in cats. This condition can affect young female cats that are pregnant or actively cycling or cats of either gender that have received progesterone-containing compounds.10,11 Typically there is rapid enlargement of multiple glands. Aspirates from affected mammary glands contain both uniform epithelial cells and spindled mesenchymal cells, usually associated with abundant pink extracellular matrix material.12 The epithelial cells are of ductal origin and have a relatively high nuclear-to-cytoplasmic ratio with dense round nuclei and a small amount of basophilic cytoplasm. The mesenchymal cells may exhibit moderate anisocytosis and anisokaryosis.12 Ovariohysterectomy or removal of the progesterone-containing compound is generally curative. Drug therapy with a progesterone antagonist has also been an effective treatment.13
Malignant Neoplasms
Mammary gland tumors are common in both dogs and cats; however, the biological behavior of the tumors varies greatly between these species. Mammary tumors comprise up to 50% of neoplasms in the bitch, and 40% to 50% of those tumors are malignant, with adenocarcinomas the most common histologic type.6,14 Mammary tumors are the third most common neoplasm in cats and account for about 17% of all neoplasms in queens.7 By contrast to dogs, up to 80% of feline mammary gland tumors are malignant. Similar to dogs, adenocarcinomas are diagnosed most frequently.15,16 Mammary tumors are rare in males of both species.6,17
Multiple morphologic types of carcinoma are recognized histologically based on the pattern of cell arrangement and degree of cell differentiation.7 Carcinomas are also graded based on histologic features such as tubule formation, mitotic rate, and cell pleomorphism. Many different types of carcinomas can contain collagenous stroma, sometimes in large amounts. Both histologic type and grade, as well as degree of invasion, have been shown to have prognostic significance in dogs.18 Dogs frequently have multiple tumors, which are often of different histologic types.14 In cats with mammary carcinomas, tumor size has been shown to be the single most important prognostic factor.16,19
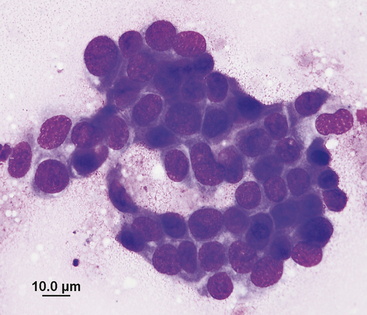
Cytologic criteria that best correlate with malignancy include variable nuclear size, nuclear giant forms, high nuclear-to-cytoplasmic ratio, variable numbers of nucleoli, abnormal nucleolar shape, and the presence of macronucleoli (Figures 6-7 and 6-8).1 However, as previously discussed, mammary malignancies may be well differentiated and show little cellular pleomorphism, and moderate criteria of malignancy may be present in tumors considered benign due to lack of tissue invasion. Smears of aspirates from adenocarcinomas generally contain epithelial cells occurring singly and in clusters of variable size. Adenocarcinoma cells are usually round, with round to oval, eccentrically placed nuclei and variable quantities of basophilic cytoplasm that occasionally contains vacuoles that may be filled with secretory product (Figure 6-9). Cell borders are usually distinct, and cells may be arranged in acinar or tubular patterns. Binucleated or multinucleated cells may be seen. Mesenchymal cells may be present in variable numbers.
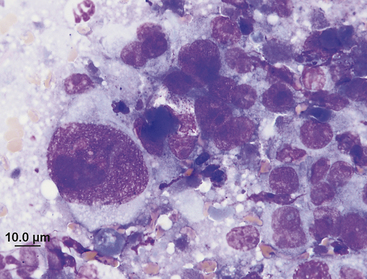
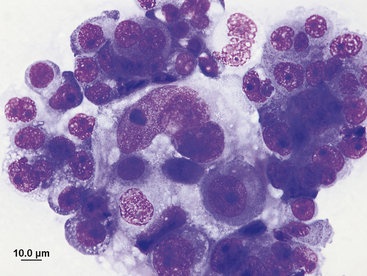
Figure 6-8 Pleural fluid from the same cat as Figure 6-7 contains tightly cohesive clusters of epithelial cells with marked criteria of malignancy, confirming the presence of intra-thoracic metastatic disease. (Wright’s stain, 1000×.)
Anaplastic carcinomas are diffusely infiltrative tumors composed of large, pleomorphic epithelial cells with bizarre nuclear and nucleolar forms.7 These cells occur singly and in variably sized clusters and have a high nuclear-to-cytoplasmic ratio (Figure 6-10). Multinucleated cells and mitotic figures are common (Figures 6-11 and 6-12). These tumors may contain abundant collagenous stroma infiltrated by inflammatory cells.7 Anaplastic carcinomas frequently metastasize and have a poor prognosis.
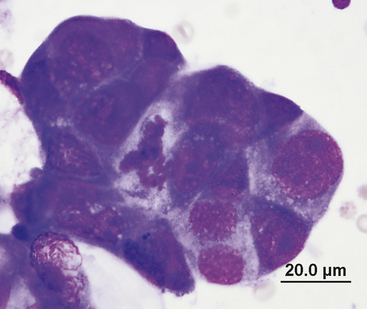
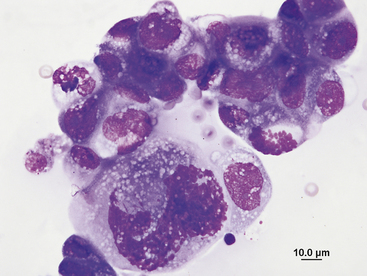
Figure 6-11 Anaplastic mammary carcinoma, same aspirate as Figure 6-10. Malignant epithelial cells have cytoplasmic vacuoles in this cluster, and two mitotic figures are present. (Wright’s stain, 1000×.)
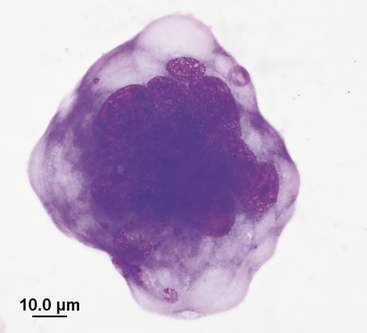
Figure 6-12 A large multinucleated epithelial cell from the same anaplastic mammary carcinoma as Figure 6-10. Notice the nuclear fragments visible in the cytoplasm. (Wright’s stain, 1000×.)
Inflammatory carcinomas have distinctive clinical and histologic features and are aggressive tumors associated with a poor prognosis. These tumors may be misdiagnosed as mastitis due to the marked inflammation and clinical signs of systemic disease. Inflammatory carcinomas have been reported in dogs and cats, with a variety of histologic types represented.20–22 In one report, cytology of mammary gland aspirates revealed malignant epithelial cells in 15 of 33 dogs and contributed to the diagnosis; the other 18 cytologic samples had low cellularity.21 The hallmark of inflammatory carcinoma was the histologic finding of dermal lymphatic involvement.21
Nonglandular carcinomas may be simple, with only epithelial proliferation, or complex, with cells of epithelial and myoepithelial origin. Accordingly, cytology samples may contain predominantly epithelial cells or a mixture of cell types. In contrast to adenocarcinomas, epithelial cells from nonglandular carcinomas may not contain intracytoplasmic vacuoles (Figure 6-13). Squamous cell carcinomas in mammary glands appear cytologically similar to those in other body regions. Tumor cells occur singly or in small sheets and may be keratinized or non keratinized. Nuclei are variable in size, from small and pyknotic to large with immature chromatin and prominent nucleoli. Cytoplasm is variably abundant and basophilic, appearing glassy and blue-green with keratinization (see Chapter 5 for further discussion of the features of squamous cell carcinoma). These tumors frequently adhere to the overlying dermis and may be ulcerated, leading to the presence of many inflammatory cells and bacteria in samples taken from ulcerated areas. It is important to realize that squamous metaplasia may occur in other tumor types; thus finding squamous cells on a cytologic sample is not specific for squamous cell carcinoma (Figure 6-14).7,8
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


