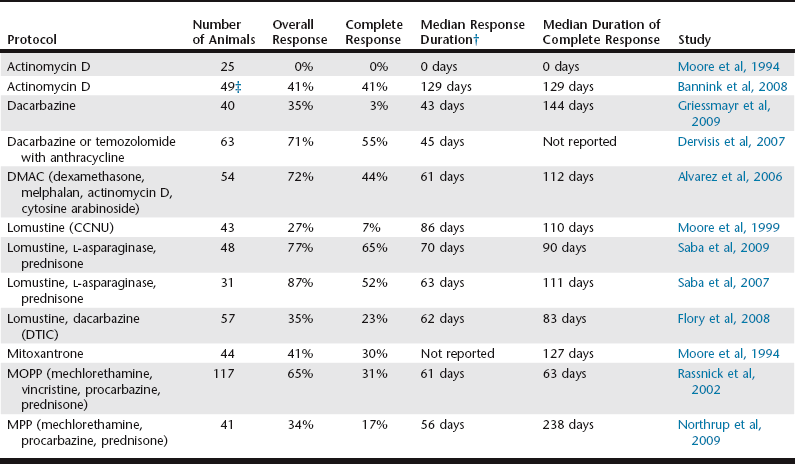
Chapter 85 At the first recurrence of lymphoma, it is recommended that reinduction be attempted, first by re-treating with the induction protocol that was initially successful, provided the recurrence occurred far enough temporally from the conclusion of the initial protocol (e.g., ≥2 months) to make reinduction successful. Attention must be given to the cumulative dose of doxorubicin that will result from reinduction, and baseline cardiac assessment, the use of cardioprotectants, alternative drug choices, and client education all should be considered. In general, the length of the reinduction is half that experienced following the initial therapy; however, a subset of animals enjoy long-term responses following reinduction, especially dogs that completed the initial induction protocol and had not been receiving chemotherapy for several months when relapse occurred. Nearly 80% to 90% rates of successful reinduction can be expected in dogs that have completed CHOP-based protocols and experience relapse while not currently receiving therapy (Flory et al, 2011; Garrett et al, 2002). The duration of the remission with a reinduction CHOP-based protocol is predicted by the duration of the interval between protocols and the duration of the first remission (Flory et al, 2011). In their study, Flory and colleagues found that 78% of dogs achieved a complete response (CR) with the reinduction CHOP protocol, and the median second remission duration was 159 days. Furthermore, dogs that had at least a 4-month remission following their induction CHOP treatment experienced reinduction remissions that were approximately twice as long as those of dogs with induction remissions of less than 4 months (214 days versus 98 days, respectively), which suggests that time off chemotherapy is an important predictor of reinduction success. This implies that dogs that experience relapse quickly after completion of their initial CHOP protocol may be better served by initiating rescue therapy immediately and bypassing reinduction altogether; however, the absolute temporal cutoff for what constitutes a “quick” relapse currently is unknown. If reinduction fails or the dog does not respond to the initial induction, the use of so-called rescue agents or protocols may be attempted. These are single drugs or drug combinations that typically are not found in standard CHOP protocols and are reserved for use in the setting of drug resistance. The most common rescue protocols used in dogs include single-agent or combination treatment with actinomycin D, mitoxantrone, doxorubicin (if doxorubicin was not part of the original induction protocol), dacarbazine, temozolomide, lomustine (CCNU), l-asparaginase, mechlorethamine, vinblastine, vinorelbine, procarbazine, prednisone, or etoposide. Some rescue protocols are relatively easy and convenient single-agent treatments, whereas others are more complicated (and expensive) multiagent protocols, such as MOPP (mechlorethamine, vincristine [Oncovin], procarbazine, prednisone). Overall rescue response rates of 40% to 90% are reported; however, responses usually are not durable, with median response durations of 1.5 to 2.5 months being typical, regardless of the complexity of the protocol. A small subset of animals (<20%) experience longer rescue response durations. Table 85-1 provides a summary of canine rescue protocols for which results have been published. It is critical to note that current published studies of rescue protocols do not include sufficient numbers of subjects for adequate statistical power, nor do they compare protocols in a randomized prospective fashion. Therefore evaluations of efficacy for various protocols are subject to substantial bias, which makes direct comparisons difficult and indeed precarious. Therefore, at present, choice of a particular rescue protocol should depend on several factors, including cost, time commitment required, efficacy, adverse event profile (i.e., toxicity), and experience of the clinician with the protocols in question. Because the complexity of rescue protocols does not yet appear to be associated with significant gains in rescue durability, the author tends to choose simpler and less costly protocols (e.g., lomustine/l-asparaginase/prednisone) (Saba et al, 2007) (Table 85-2). That being said, the use of multiple varied rescue protocols, altering as needed based on response and continuing as long as clients are comfortable with the quality of life of their dog, is commonplace. This sequential application of several different rescue protocols can result in several months of extended survival with acceptable quality of life. TABLE 85-1 Summary of Response Data for Rescue Protocols in Dogs (Tested in a Minimum of 25 Animals)* *Few of these studies tested protocols in sufficient numbers of subjects for adequate statistical power, and even fewer compared treatment protocols in a randomized prospective fashion. In addition, staging, inclusion, and response criteria varied considerably among studies listed. Therefore evaluations of efficacy between the various protocols are subject to bias, which makes direct comparisons difficult. †Various temporal response end points were used, including disease-free interval, time to progression, and progression-free survival.
Rescue Therapy for Canine Lymphoma
Reinduction Chemotherapy
Rescue Chemotherapy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


