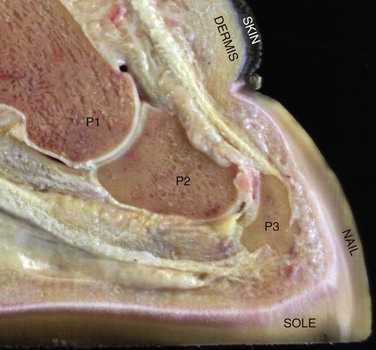
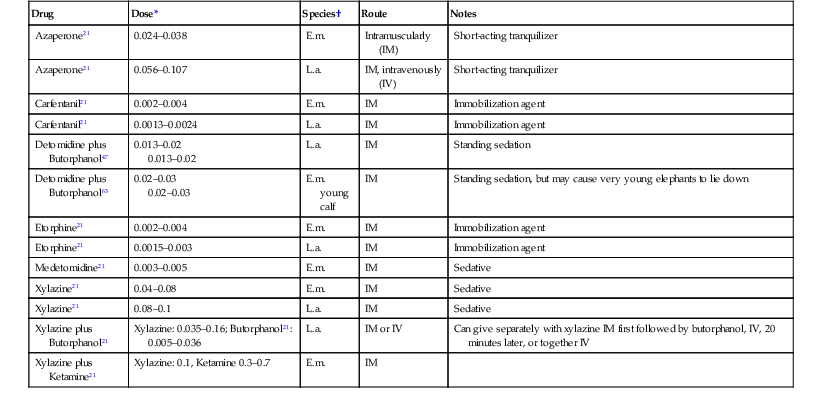
Ellen Wiedner As the largest extant land mammal, the elephant is characterized not only by great size but also by extraordinary intelligence, complex social behavior, and its remarkable nose, capable of uprooting large trees or grasping single grains of rice. Over the past 4000 years, elephants have been worshipped as gods, used as work animals and beasts of war, and admired in zoos and circuses. However, elephants now face an uncertain future. The growing demand for ivory has decimated herds in both Africa and Asia, and human–elephant conflicts, ongoing habitat loss, demand for bush meat (African elephants), skewed sex ratios because of ivory poaching (Asian elephants), and politics have caused further massive losses of elephant populations. The captive population is not self-sustaining, and the extinction of elephants—a horrific thought—could become a reality in the not-so-distant future. Elephants are an ancient species that are placed in superorder Afrotheria, clade Paenungulata, order Proboscidea. Probscideans first appeared in Africa during the early Cenozoic period, approximately 60 million years ago, but these early ancestors were not much larger than a golden retriever and bore little resemblance to modern elephants. Characteristics such as gigantism, the long dexterous trunk, and the distinctive tusks and molars evolved over millions of years as the group migrated into Europe, Asia, India, and the Americas. The taxonomy and classification of the proboscidea continue to be debated, but currently only modern elephants (Loxodonta and Elephas), mastodons (Mammut), and mammoths (Mammuthus) are placed together in the family Elephantidae. Woolly mammoths (M. primigenius), the last of the ancestral elephants, became extinct 5000 to 10,000 years ago. The closest living relatives to elephants are other members of the Paenungulata: the order Sirenia (manatees and dugongs), and the order Hyracoidea (rock hyraxes). Evidence for these relationships may be found in the fossil record, in genetic and immunologic studies, and in comparative anatomic data.56 Today, two genera of elephants are recognized, Loxodonta and Elephas. Genus Loxodonta, the African elephant, includes two species: L. africana, the African savanna elephant, and L. cyclotis, the forest elephant, although L. cyclotis is not universally accepted. Genus Elephas, the Asian elephant, includes a single species, E. maximus, but some zoologists recognize a variety of subspecies, including E. m. sumatranus, E. m. indicus, and E. m. maximus. This too is controversial.56 Both L. africana and E. maximus share the same number of diploid chromosomes (n = 56). In nature, the two species are so geographically separated that interbreeding is impossible. However, one known African–Asian hybrid was born in captivity, the calf “Motty,” born at the Chester Zoo in 1978, to an Asian elephant mother and an African elephant father. Motty lived less than 2 weeks before dying of necrotizing enterocolitis, but was confirmed to be a hybrid with testing of tissues samples.31 Table 53-1 provides a comparison of African and Asian elephants. TABLE 53-1 Comparison of African and Asian Elephants56 Elephants are long lived, often reaching their 40s in the wild and their 50s and 60s in captivity.72 They are a herd species, with an intricate social structure and multiple communication systems. These systems include complex vocalizations, infrasound (sound below the range of human hearing),23 and chemical signaling via hormones, proteins, and volatile compounds released in urine, feces, breath, and secretions from specialized glands such as the temporal gland, a unique Proboscidean apocrine gland located on each side of the head. These bioactive compounds transmit information about the individual’s reproductive status, territory, and dominance and likely about other aspects of elephant society both within and without the herd.50 Elephant habitats are highly varied. For African elephants, this includes environments that range from hot deserts to savannas, as well as dense forests and wetlands at a variety of altitudes. Asian elephants are found in similarly diverse habitats that also include shrub land, wet and dry forests, evergreen and deciduous woods, and degraded areas. The International Union for Conservation of Nature (IUCN) Red List of Threatened Species classifies Loxodonta as vulnerable but comments that the status is regionally variable. Asian elephants are classified as endangered. Both species are listed in the Convention on International Trade in Endangered Species I (CITES I) Appendix. From one end to the other, the elephant’s anatomy is highly unusual, starting with the proboscis—or trunk—which is the obvious example. Thickly muscled, extremely flexible, and complexly innervated, the trunk is comparable to a hand. In fact, the fingerlike appendages on the distal trunk (single in Elephas, double in Loxodonta) are densely packed with Pacinian corpuscles and vibrissae, which enable both refined grasping of small objects and discrimination of diverse sensory stimuli.50 Since the elephant is unable to lower its head to the ground while in a standing position and has little movement of its neck compared with other species, the trunk is essential for bringing food and water to the mouth. Elephants also use the trunk as a weapon, to toss dirt and sand on their backs, to spray water, and for communication with herdmates both by tactile means and by bringing chemically active substances to the vomeronasal organ located on the dorsal surface of the mouth.51 The tusks are upper incisors, present in both genders of African elephants but only in males in Asian elephants. Female Asian elephants often have rudimentary tusks called tushes. Tusks grow continuously throughout an elephant’s life. For a very brief period after they erupt through the sulcus, they are covered in shining white enamel. When the enamel is shed, what remains underneath is the off-white dentine, the substance known as “ivory.” Primary dentine is on the outside of the tusk. Secondary dentine is laid down within the pulp cavity; thus, the diameter of the elephant tusk increases from the interior.16 The great preference for elephant ivory over that of other species is because of several unusual characteristics. First, elephant ivory is softer than most other ivories; second, it cracks less easily, and finally, in cut section, its arrangement of overlapping dentine tubules creates subtle checkerboard effects. These are called Shreger patterns and are unique to the proboscideans. They give elephant ivory its great beauty when carved.58 Tusks grow approximately 18 centimeters (cm) a year and, in large African males, may reach more than 3 meters (m) in length and 70 to100 kilograms (kg) in weight.58 In the center of the tusk is the pulp cavity, which is filled with blood vessels, nerves, and growing cells. Over time, as the tusk elongates, the most distal part of the pulp cavity becomes compressed and atrophied. On cross-section, this atrophied tissue may be seen as a black dot in the center of the tusk and should not be confused with the actual pulp cavity. The absence of tusks (natural tusklessness) is a female sex-linked trait. When wild populations of either Asian or African elephants are heavily poached for ivory, this trait emerges. When poaching decreases, tusklessness diminishes.59 In most of Asia, tuskless males are called “makhnas.” The molar formula is: incisors (I) 1/0, canines (C) 0/0, premolars (P) 3/3, molars (M) 3/3, although some authors consider all cheek teeth to be molars, which would change the formula to: I 1/0, C 0/0, PM 0/0, M 6/6.37 However, all of these six cheek teeth are not present at the same time in the mouth but erupt successively over the course of the animal’s life. At any moment in time, usually only two functioning molars are present in any quadrant of the jaw. New molars are formed in alveolar pockets at the back of each jaw and are composed of compressed plates of enamel-wrapped dentine (called laminae or lamellae), which are joined together with cementum. Over time, old worn molars move forward in the jaws, dissolve their roots, and fall out of the mouth to be replaced by newly formed molars that have advanced cranially from the alveolar pockets to come into wear. This continuous process bears some resemblance to an escalator’s motion. Techniques to determine an elephant’s age by analysis of the wear and number of dental lamellae have been described but involve a large margin of error. Some elephants are not toothless at death, even if they live to an advanced age because molars 6 (M6), the last molars, are not always shed, although they may become extremely worn and fragmented.37 Neonates may be born with M1 and M2. If not present at birth, M1 and M2 usually erupt shortly thereafter and are shed by age 2 or 3 years.37 Milk tusks (also known as tushes) on young elephants, which sometimes never erupt, are resorbed and replaced by permanent tusks between 6 months and 1 year. Elephants do not have lacrimal puncta, lacrimal glands, or a nasolacrimal drainage system. Nevertheless, elephants do produce tears from multiple adnexal glands which, because of the absence of the duct system, regularly—and normally—run down the side of the face from the medial canthus.74 The pleura of elephants is represented by thick, diffuse connective tissue that attaches to ribs, diaphragm and lungs and obliterates the pleural space. This tissue is simply pleural membranes that became adhered and thickened, a phenomenon that occurs in utero, early in gestation. Containing mostly collagen fibers and having a slippery, compliant consistency, it slides and moves and still acts functionally as a pleural membrane. Although these unusual pleura attach the lungs to the chest wall, they do not appear to hamper chest wall excursions.64 The thorax is also the site of two mammary glands; elephants have breasts, not an udder. The heart may weigh more than 20 kg in an adult elephant. The cranial vena cava is paired, and the caudal vena cava is single. Numerous arteriovenous anastomoses as well as arterial and venous plexuses may be found throughout the body.45 The veins have multiple valves that likely cause some of the difficulties can be experienced when drawing blood. These valves, plexuses, and anastomoses are related to the complex—and poorly understood—hydraulics involved in moving the massive blood volume around the elephant’s body. Elephants lack a gallbladder but have a duodenal pouch that connects both the biliary and pancreatic ducts.45 The liver is unusual in that it produces C27 bile alcohols rather than bile acids, a characteristic shared with other Paenugulates as well as with some cartilaginous fish. Unlike bile acids, which lose their taurine conjugate when bacteria bind to them, bile alcohols lose a sulfate conjugate. This characteristic renders them insoluble across lipid bilayer membranes and traps them within the bile ducts. These trapped bound bile alcohols are believed to predispose elephants to cholelith formation.2 Elephants are hind gut fermenters with a simple stomach. The small intestines terminate at a large sacculated, conical cecum, which, in turn, connects to a partially sacculated large intestine. Microbial fermentation of feed begins in the small intestine, peaks in the cecum, and continues in the colon. Elephants have short intestines and rapid gut transit times, which lead to lower digestibility coefficients compared with those in domestic hoofstock and are a measure of the amount of nutrition taken in from a particular feed.14 Elephant kidneys are reniculate and are composed of 6 to 10 lobes, some of which may be fused. In most adult elephants, urine does not concentrate significantly, even if the animals have not drunk water for a while; this may be explained, in part, by the anatomy of the kidney, which includes small or absent renal papillae and minimal contact between urine and the outer renal medulla at the calyx.66 The elephant’s foot is adapted to support its great weight. The circumference of the forefeet is greater than that of the hindfeet. Foot anatomy is similar in both Asian and African elephants, although minor differences exist in appearance with regard to the number of toenails. The nails are not weight bearing and grow less than 1 cm per month. They are connected to the underlying phalanges by laminae.46 All feet have five digits regardless of the number of nails present. By convention, the digits are numbered DI through DV, with the most medial digit always being DI. Each digit consists of three (sometimes two) phalanxes and one metacarpal or metatarsal. DIII is the longest. Because of the vertical arrangement of the metacarpals, they provide equal weight support at the front of the body, whereas the metatarsals are more horizontally organized, resulting in the majority of weight being carried by DII, DIII, and DIV.46 The bones of the feet sit atop a digital cushion composed of fat and connective tissue, which acts as both shock absorber and fluid pump.8 With every step the elephant takes, the cushion compresses and deforms outwardly causing the circumference of the foot to expand. Additionally, compression of the cushion helps push blood from the feet back to the heart, another hydraulic adaptation. A cartilaginous prepollux and prehallux in the forefeet and hindfeet, respectively, create subcompartments within the cushion and also act as struts for the foot.46 The bottom of the foot, sometimes called the slipper, consists of the sole (the underside of the toes) and pad (the underside of the foot) and is composed of horny, keratinized tissue. This keratinized material grows from an underlying germinal epithelium, which, in turn, sits atop the sensitive corium. The slipper is quite thin, rarely more than 4 to 12 millimeters (mm) thick, and is usually corrugated in adults.8 (Figure 53-1). Elephants are herd animals and generally require contact with other elephants. Housing should provide space for social interactions and also room to separate the elephants that are not getting along with the others or for medical reasons. Housing may be as simple as a basic shelter offering protection from the elements in warm climates or a sophisticated modern barn with a temperature-controlled environment and hydraulic gates. Good ventilation, ability to thoroughly clean the facility, and construction materials that cannot be destroyed by the elephants are of paramount importance. A variety of flooring surfaces has been used in elephant housing, but it remains unclear what type of floor is best. Smooth floors, roughened floors, deep sand pits, and specialized polymers have all been used. In some facilities, elephants have pulled up and ingested newly installed floors, so durability is an important consideration. Outdoor facilities may consist of multiple yards or a single communal yard. Generally, female elephants share paddocks, whereas each male is kept separately. Some facilities have incorporated all of their elephants, young, old, male, and female into herds that share a yard. Because elephants protect their skin by throwing dirt and sand on their backs, access to these materials is necessary. Swimming pools, waterfalls, and ponds are enjoyed by elephants but should be easy to clean and quickly drainable in case of emergency. Pools do not need to be deep, and, in fact, many elephants enjoy playing in just a few inches of water. Filtration systems must be installed out of reach of the elephants. The size of the yard needed is debatable. The majority of wild elephants, both African and Asian, tend not to move around very much at all, maxing out at 5 to 10 km per day.40 The only elephants that have been shown to walk long distances, up to 30 miles per day, is a unique group of African elephants living in the extremes of the Namib desert where drought and inadequate food sources make the terrain inhospitable.62 However, regular exercise does benefit captive elephants as it decreases foot problems, improves heart health, and provides enrichment. Thirty minutes of exercise per day is likely a reasonable goal that may be achieved by walking the animals, encouraging a variety of stretching moves, or both.65 Healthy elephants may be acclimated to a wide range of temperatures. Elephants living in northern climates will often freely choose to play in snow and even break ice on ponds to go swimming. Precipitation, wind chill, and scarcity of sunshine may, however, decrease the tolerance levels of the elephants for cold weather. In very hot environments, appropriate shade structures and water are obviously important, as is sand or dirt for dust bathing. Toys and enrichment devices should be too big to be swallowed, difficult to destroy, and of sufficient interest to the elephants. Heavy large plastic balls, rubber motorcycle and truck tires, and knotted firehose have been used. Several facilities have installed fake trees where food items are hidden so that elephants spend time searching for them. Facilities that house bull elephants have additional safety considerations. All institutions holding elephants require adequate perimeter fencing and containment, but those with bulls need containment that should withstand the aggressive behavior of a male in “musth” (a period of hormone-induced aggression). An elephant restraint device (ERD) is recommended and even required at facilities accredited by the Association of Zoos and Aquariums (AZA). An ERD is a large chute that enables restricted contact and close-up handling of any elephant. ERDs come in a variety of configurations, but all permit access to the feet, legs, and head of the elephant via movable gates and may be adjusted to hold elephants of different sizes for the duration of a particular procedure. Some ERDs have a scale built into the floor so that the elephant may be weighed each time it enters the device. Others have incorporated tilt tables. In Asia, elephant camps often have wooden stocks, built of large tree trunks that function like an ERD. Whatever the conformation of the ERD, the elephant needs to be conditioned to it and trained to go in and out reliably. Breeding facilities need to baby-proof their barns and yards. As Rudyard Kipling noted, little elephants have “ ’satiable curiosity.” Considerations include keeping the calf from escaping, since calves may wiggle through very small vertical gaps. Pools may need to be lowered or emptied until it has been ascertained that the calf can swim. In the wild, elephants are browsers and grazers, demonstrating great diversity and selectivity in the foods they eat. They tend to feed throughout the day, rather than eat discrete meals. In general, the natural diet for both African and Asian elephants contains high amounts of fiber and relatively low amounts of protein (8% to 12%). Wild elephants eat approximately 1.2% to 1.9% of their body mass in feed volume daily. Currently, their daily energy requirements are unknown.27,65 Captive elephants in Asia are commonly fed palm leaves, bark, rice, tamarind, balls of salt, and green fodder and may be routinely released into nearby forests to browse. Captive elephants in the western hemisphere are typically fed diets of hay, browse, pellets, grains, fruits, vegetables, and miscellaneous items, ranging from bread to beet pulp. Some facilities provide pasture access to their animals. Many North American facilities successfully feed their elephants hay and browse diets without adding commercial pellets, which tend to be low in fiber and high in protein.65 Regular forage analysis by a reputable laboratory is strongly encouraged because hay quality and nutrients may vary. Weighing feedstuffs and standardizing the diet are also recommended. Feed needs to be stored properly, away from weather and vermin. Caretakers should be educated about hay quality, nontoxic species of browse, and appropriate storage procedures. Variability in browse may provide enrichment, high amounts of fiber, and appropriate abrasiveness for teeth. Regular weighing of elephants should be part of all captive programs. The use of weight tapes has been described in elephants, but a scale provides better accuracy. Published guides to elephant body condition scoring are available but often fail to describe overweight elephants or acknowledge variations in body type. Accurate assessment of body condition requires gaining experience with different elephant body types as well as typical changes in shape over an elephant’s life. With advancing age, gravity and conformation may cause significant alterations in appearance that should not be confused with pathology.65 Obesity in captive elephants is linked to various health problems, including reproductive abnormalities, heart disease, and osteoarthritis. Several institutions have successfully put their elephants on a diet by feeding lower-energy forages, increasing browse, and eliminating pellets and other concentrates. Gradual weight losses of 450 kg have been achieved in elephants over an 8- to 12-month period.27,65 Like all animals, elephants require adequate amounts of clean water. Although elephants have been reported to drink vast quantities of water at a single time (up to 100 liters [L]) and over the course of the day (up to 225 L), most elephants do not drink this much and will vary their intake. Some will go several days without drinking without ill effects.65 Nevertheless, in captivity, refusal to drink is often an early sign of illness and should be evaluated. Some facilities offer water on a continuous basis; others provide water to their elephants at specific times of the day. Either system is appropriate as long as keepers have the ability to observe intake. If this is not possible, urine output should be noted. This too may vary by individual.65 Working with elephants requires consideration for the safety of the animal, the handler, and the facilities. Nobody should ever go up to an elephant without the express permission and assistance of an experienced handler who is familiar with the animal. Elephants are hierarchical and generally ignore the commands of those they do not know. Because of their strength, speed, and intelligence, they may also be extremely dangerous. Safety is of paramount concern in an elephant barn. Any work with captive elephants uses training in conjunction with two different methods of handling: (1) nonrestricted contact, in which the elephant and the handler share space, and (2) restricted contact, in which the elephant and the handler do not share space or, if they do share space, the elephant is tethered. The use of either restricted or nonrestricted contact requires adequate training of both elephant and handler. In range countries, captive animals are handled almost entirely in nonrestricted contact. Circuses and organizations that use performing elephants also rely extensively on nonrestricted contact. Zoologic and breeding facilities generally use a combination of techniques that depend on the situation, the animal, and the experience of the handlers. The AZA has mandated the use of restricted contact in all AZA-accredited facilities in North America by 2014, with exceptions made for specific situations requiring direct access to the elephants. Training for these exceptions is also needed. Tools used for elephant restraint include leg restraints or tethers and a guide, formerly known as an ankus or bullhook. The guide is a stick, made of metal, wood, or fiberglass with a prong at the end. The prong is tapered into a point that may push or pull at skin but not so sharp that it breaks the skin. The guide has been highly politicized by some who maintain that its only purpose is to beat and abuse elephants. It goes without saying that this is an entirely inappropriate use of this—or any—tool. In truth, the guide acts as an extension of the human arm to enable the handler to direct the animal to move in a desired direction. The AZA, the Elephant Managers Association (EMA) and the American Veterinary Medical Association (AVMA) all recognize the guide and tethers as appropriate tools in elephant management. Typically, elephants are trained for a variety of minor medical and husbandry procedures. However, elephants are sometimes not cooperative when they are ill. In other situations, young elephants may not be reliably trained, and bull elephants, whether in musth or not, may be unpredictable. In these situations, chemical restraint or general anesthesia may be helpful. For surgical procedures, chemical restraint with analgesia is a necessity. Chemical restraint may be achieved by standing sedation or general anesthesia in lateral recumbency, with or without gas anesthesia. It is necessary to remember that elephants often have unexpected responses to anesthetic agents, which have to be used with great care and sensitivity; chemical restraint therefore has to be approached as both art and science. Discussing protocols beforehand with veterinarians experienced in sedating and anesthetizing elephants is recommended. Elephants sometimes go down into sternal or even lateral recumbency with a standing sedation protocol. Facilities should prepare in advance for this possibility by having reversal agents available and should perform the procedure at a location where the animal may go down without getting injured. Drugs typically used for standing sedation including α2-agonists, often combined with butorphanol. Azaperone has been used as a short-acting tranquilizer both by itself and with butorphanol added. Ultrapotent narcotics are typically used for general anesthesia.21 Etorphine is preferred over carfentanil. Both halothane and isofluorane have been used to maintain anesthesia following endotracheal intubation. Various local anesthetics have been used in elephants. Use of adequate local anesthesia may sometimes decrease or obviate the use of other sedatives. However, infiltration of the drug may be extremely difficult because of the thickness of the skin. Some of these agents may, however, work well on mucous membranes.21 Table 53-2 lists drugs and doses for sedation and immobilization of elephants. Box 53-1 lists reversal agents. The reader is strongly encouraged to consult some of the recent textbooks and literature on elephant sedation and anesthesia prior to any sedation procedure. TABLE 53-2 Doses for Sedating and Immobilizing Elephants * Doses are in milligram per kilogram (mg/kg) unless otherwise stated. † E.m., Elephas maximus; L.a., Loxodonta africana. Obtaining the accurate weight prior to drug administration facilitates safer anesthesia. In wild elephants, this is obviously not possible. Overdosing of drugs given for standing sedation is certainly a risk factor for an elephant falling. In wild animals, higher doses are used because the animals are less calm to begin with. However, underdosing is equally disadvantageous as it may cause excitement, incoordination, and ataxia. Frequent redosing may be dangerous and result in unwanted effects. Drug delivery may be performed by hand injection in a well-trained elephant or with darting equipment. Drugs should be delivered into the triceps, upper muscles of the thighs, or gluteal muscles using long needles (at least 5 cm) to ensure intramuscular administration. Pole syringes or jab sticks should not be used in elephants that are not enclosed within an ERD, since they may turn quickly and grab the device from the handler. Wild elephants are typically darted using power-charged projectors, often from a helicopter.21 For elective surgeries, elephants should be fasted 24 to 48 hours prior to anesthesia, and water should be withheld for 24 hours. Appropriate padding is needed to prevent peripheral nerve damage and compartment syndrome while the elephant is in lateral recumbency. Multiple large and thick mattresses or specially crafted waterbeds may be used. Bolsters or large inner tubes should be placed between the legs.18 In a captive setting, elephants may be trained to lie down on command. If so, anesthetic drugs may be directly injected in the awake, recumbent animal, which avoids the elephant falling and being injured during induction. If this is not possible, a system of ropes or a sling may be used to pull the elephant into recumbency.76 Site hazards such as moats, pools, and parked equipment should be evaluated beforehand and altered, if needed.18 Following induction, intubation may be done using a 30- to 50-mm internal diameter (ID) cuffed endotracheal (ET) tube in an adult, a 12- to 16-mm ID tube in a newborn calf. The elephant’s mouth may be pulled open with cotton ropes and a bite block placed between the upper and lower molars on one side of the jaw prior to intubation. Another technique is to place a strap around the lower jaw and attach it to a rope running between the animal’s front legs.76 Intubation is done blindly with the use of a 2-m stylet or an equine stomach tube used as a guidewire. With one’s gloved arm inserted into the back of the throat, the soft palette is pushed upward to access the epiglottis. The ET tube is then slipped over the stylet or tube into the trachea. The external portion of the ET tube may be taped to the trunk.18,76 A single large animal ventilator may be adequate in a young calf. Multiple large animal ventilators may be attached together in parallel to provide adequate tidal volume in adults. A few elephant-specific ventilators are also available, some of which have been developed for field use.76 Monitoring of the animal under anesthesia may include pulse oximetry, capnography, electrocardiography (ECG), blood gas analysis, and blood pressure measurement. Hypotension may be significant in anesthetized elephants. Pharmaceutical agents that have been used to combat this problem include ephedrine and dobutamine. Circulatory support may also be provided with intravenous fluids. Hypertension and pulmonary edema (“pink foam syndrome”) have been reported in wild African elephants following opiate anesthesia, but adding azaperone to the etorphine in a dart may be protective.76 In the past, complications reported with elephant anesthesia were numerous and included injury during induction, including tusk and bone fractures, respiratory and lactic acidosis, apnea, bloat, hypotension and hypertension, nerve damage, prolonged recovery, cardiac arrhythmias, hypoxemia and death.18,76 In recent years, with the increased experience of veterinarians in the use of a variety of anesthetic drugs and protocols, elephant anesthesia has continued to improve in safety. Surgery on elephants is often fraught with complications. Even a seemingly minor procedure such as suturing a laceration has the potential to go drastically wrong because elephants tend to open incision sites, destroy suture lines, eat bandages, and pack dirt, mud, and other debris into wounds. Conservative treatment such as cold hosing and flushing, use of topical therapies, and systemic antimicrobials often is surprisingly successful in healing even large skin wounds. Abdominal surgeries such as cesarian sections and colic surgeries on adult elephants have been unsuccessful because of difficulties in obtaining adequate access to surgical sites as well as in manipulating the massive viscera. In addition, the thickness and toughness of the skin make both opening and closing incisions extremely difficult. Other complications include incisional dehiscence and surgical infection.70 However, cesarian sections done for the purpose of removing dead calves are no longer performed because no animal has survived the procedure and also, more remarkably, because several pregnant elephants at multiple institutions have kept dead, full-term calves in their uterus for years without becoming septic. When the calves were finally passed, the bodies were neither mummified nor macerated.28 In the past several years, laparoscopic tools have been constructed specifically for vasectomies on wild African elephants. Multiple adult bulls were vasectomized without complications with the use of a sling to maintain the anesthetized animals in the vertical position.61 Vestibulotomy, or episiotomy, in which a large incision is made below the rectum to remove a dead calf from the birth canal, is another surgical reproductive procedure, which, however, has frequently resulted in poorly healing or nonhealing incisions.28 The most commonly performed surgeries in elephants are dental surgeries. Procedures on fractured tusks include extraction, pulpotomy, and pulpectomy. These entail general anesthesia and specially crafted, elephant-sized dental equipment, along with experienced personnel.16 However, conservative therapy with antibiotics and flushing and radiography to monitor progress have sufficed for some animals with broken tusks, even though the pulp cavity was open. One tusk extraction was performed by using rubber elastic bands that were advanced proximally, a little at a time each day, up the tusk of an unanesthetized elephant. This resulted in progressive loss of alveolar bone so that the tusk dropped from the sulcus in less than 1 month.60 Impacted molars usually require surgery. Molar disease may cause anorexia or colic because of difficulty masticating food. Molar removal is complicated, however, sometimes necessitating cutting the tooth into sections prior to removal. An experienced elephant dentist should be consulted about complex dental issues. Several procedures formerly done with some frequency are now rarely performed or not at all. An example is surgical castration of adult bulls, which was found not to decrease or only minimally decrease aggressiveness or musth. Surgical artificial insemination (AI) is also infrequently performed because of the growing experiences and success of zoo veterinarians with endoscopic AI. Uncommonly performed surgeries in elephants include esophagostomy, tail amputation, trunk reattachment (unsuccessful), fracture repairs, biopsies of various tissues and organs, cataract surgery, umbilical hernia repair, temporal gland extirpation, and tumor removal. Elephant necropsies warrant mention here. They may be difficult, time consuming, and emotionally taxing but may add greatly to general knowledge about elephants as well as about specific issues in a collection of animals. Necropsy guidelines may be found on the AZA website. Having an experienced pathologist available for consultation and preferably direct assistance may be very helpful. A team approach is needed for an elephant necropsy. These include individuals to do the actual gross dissection, heavy machinery operators, and personnel to label and process tissue, sharpen knives, and record data. Prior to starting, the team should discuss how detailed the necropsy will be, review safety protocols for large cutting tools and heavy equipment, and discuss record keeping, sample collection, and submission. Disposal of the carcass should be determined in advance, whether it should be field burial or cremation. Another consideration at a necropsy is potential exposure to tuberculosis (TB) or other zoonotic diseases. Personal protective equipment includes gowns, gloves, boots, face shields, and respirators specifically designed to protect against aerosolized microorganisms (N-95 facemasks at a minimum). Surgical masks are not appropriate protection. Typically, the thorax is opened last, and if suspicious granulomatous lesions are present anywhere in the respiratory tract, the number of personnel is minimized, protective gear is donned, and power tools are avoided to decrease possible aerosolization. Multiple samples should be collected quickly and packaged securely. Any further manipulation of the carcass should be done only as needed for disposal and with minimal exposure of tissue. Scant pharmacologic studies have been performed in elephants, so clinicians are often left to extrapolate doses for elephants from those published for domestic hoofstock. Three techniques have been described: linear scaling, metabolic scaling, and allometric scaling. The first two techniques are seldom appropriate for elephants and have the most potential to result in significant overdoses and toxicity. Linear scaling simply inserts the weight of an elephant into a milligram-per-kilogram (mg/kg) dose established for another species. This method assumes that the pharmacokinetics are identical between the two species and that a linear scaler is adequate. As a result, linear scaling tends to vastly overdose larger animals. The metabolic scaling technique factors in a physiologic estimate such as metabolic rate. Because the scalar is nonlinear, the dosage estimates may be more accurate for larger animals, but identical pharmacokinetics between both species are still assumed. However, several papers have demonstrated that elephant pharmacokinetics are different from horse or cow pharmacokinetics and that this technique also fails to predict accurate dosages. The last technique, allometric scaling, is probably the most appropriate with regard to elephants but requires having pharmacokinetic data from multiple species about drug half-life, clearance, and volume of distribution which may be plotted against body weight. Drugs most appropriate for allometric scaling are those that have blood flow–dependent clearance. This includes only a select few drugs, primarily antibiotic agents. Even when pharmacokinetic studies are done in elephants, they do not address pharmacodynamic issues, that is, how the drug behaves in the body—its efficacy, safety, and toxicity. In fact, many pharmaceutical agents cannot be safely extrapolated for use in elephants for reasons that include differences in elephant liver and kidney physiology, drug conjugation mechanisms, and underlying metabolism. An excellent discussion of the issues involved in drug dose extrapolation to elephants may be found in the article by Hunter and Isaza.32 Elephants may be medicated through a variety of routes. Oral administration is ostensibly the most straightforward technique, but elephants are highly sensitive to unpleasant tastes and may refuse medications or spit them back out, even if mixed into pleasant-tasting substances such as honey or syrup. Elephants may be trained to use a bite block, but the author has had the experience of medicating an elephant orally with a bite block, watching the animal seeming to swallow and even eat hay for over 2 hours, and then surreptitiously spitting out the entire dose of pills in a corner of her pen. Intramuscular injections into the triceps or thigh muscles also require training. Repeated administration of drugs intramuscularly (IM) is apt to be painful and result in abscess or scar tissue formation. This is a concern if long-term therapy is needed. The use of longer-acting formulations of various antibiotics may be considered, although they too may cause large swellings at the site of injection. Intravenous administration of drugs should be avoided unless an intravenous catheter has been placed either in an ear or saphenous vein. Several elephants have sloughed off large portions of their ears because of intravenous drugs leaking extravascularly. In addition, it is not always easy to distinguish between an artery and a vein in the ear, and some of the ear sloughing has been the result of vessel misidentification. Intravenous catheters, however, may be tricky both to place and to maintain in elephants and are subject to thrombosis, hematoma formation, thrombophlebitis, and loss of patency. Elephants also remove them with their trunks. Giving large volume of fluids via intravenous catheter for circulatory support is often difficult as well. Furthermore, because elephant serum osmolarity is extremely low, all commercially available fluids are hyperosmotic to the serum. This has unknown clinical significance.25 Subcutaneous administration into the folds of the neck is a possibility, but very few drugs have been evaluated using this route. Another route of drug administration in elephants is via the rectum. The elephant rectum is highly absorptive, and if the elephant is trained for allowing rectal ultrasonography, rectal drug administration may also be done. Prior to drug administration, feces should be manually evacuated from the rectum. The drug should be mixed with warm water until dissolved in a large dosing syringe with a piece of soft rubber tubing attached. The syringe with attached tubing should be deposited into the rectum as far as the arm can reach before depressing the plunger. In addition, large volumes of plain water may also be given rectally for circulatory support. Elephants appear to absorb what they need by this method and excrete the rest. Rectal fluids may be given using a bilge pump or a garden hose turned to a moderate rate and a lukewarm temperature. Fluids should be turned off if the elephant strains, and turned back on when the rectum relaxes. Retention may be aided by holding the tail down firmly after administration.67 Table 53-3 lists drugs used in elephants in which the pharmacokinetics were studied, Numerous reports exist of empirical dosing. For the reasons cited earlier, caution is advised. TABLE 53-3 Selected Pharmaceutical Agents Studied in Elephants
Proboscidea
General Biology
Parameter
Loxodonta
Elephas
Weight
4000–7000 kilograms (kg)
2000–5500 kg
Height
–4 meters (m)
2–3.5 m
Dorsum
Upward slope toward rump
Downward slope toward rump or no slope
Head
Single large bulge on forehead
Two large bulges on forehead
Forehead concavity develops with age
Ears
Very large and hang below neck
Smaller
Molars
Diamond shaped occlusal surface
Narrow loops on occlusal surface
Tusks
Tusks present in both sexes
Tusks only in males
Females have vestigial tusks (tushes) or none
Unique Anatomy
Special Housing Requirements
Feeding
Restraint and Handling
Drug
Dose*
Species†
Route
Notes
Azaperone21
0.024–0.038
E.m.
Intramuscularly (IM)
Short-acting tranquilizer
Azaperone21
0.056–0.107
L.a.
IM, intravenously (IV)
Short-acting tranquilizer
Carfentanil21
0.002–0.004
E.m.
IM
Immobilization agent
Carfentanil21
0.0013–0.0024
L.a.
IM
Immobilization agent
Detomidine plus
Butorphanol47
0.013–0.02
0.013–0.02
L.a.
IM
Standing sedation
Detomidine plus
Butorphanol63
0.02–0.03
0.02–0.03
E.m. young calf
IM
Standing sedation, but may cause very young elephants to lie down
Etorphine21
0.002–0.004
E.m.
IM
Immobilization agent
Etorphine21
0.0015–0.003
L.a.
IM
Immobilization agent
Medetomidine21
0.003–0.005
E.m.
IM
Sedative
Xylazine21
0.04–0.08
E.m.
IM
Sedative
Xylazine21
0.08–0.1
L.a.
IM
Sedative
Xylazine plus Butorphanol21
Xylazine: 0.035–0.16; Butorphanol21: 0.005–0.036
L.a.
IM or IV
Can give separately with xylazine IM first followed by butorphanol, IV, 20 minutes later, or together IV
Xylazine plus
Ketamine21
Xylazine: 0.1, Ketamine 0.3–0.7
E.m.
IM
Surgery
Pharmaceuticals
Drug
Species*
Dose†
Route
Notes
ANTIBIOTICS
Amikacin42
L.a.
6.0–8.0
Intramuscularly (IM) q24h
Tested in 2 healthy elephants
Amoxicillin55
E.m.
11.0
IM, q24h
Tested in 5 healthy elephants
Ampicillin53
E.m.
8.0
Orally (PO), q8or 12h
Single dose tested in 3 healthy elephants
Ceftiofur (short acting)15
E.m.
1.1
1.1
IM, q8 or 12h
IV, q24h
Tested in 4 healthy elephants
Ceftiofur (long acting)1
E.m.
6.6
Subcutaneously (SC), q7-10d
Tested in 11 healthy elephants
Enrofloxacin54
E.m.
2.5
PO, q24h
Tested in 6 healthy elephants
Metronidazole24
E.m.
15.0
Rectally, q24h
Tested in 1 sick elephant
Oxytetracycline (long acting)12
L.a.
18.0
IM, q48h
Tested in 18 healthy elephant calves
Benzathine Penicillin G and Procaine Penicillin55
E.m.
4,545.0 international units per kilogram (IU/kg)
IM, q24, 48, or 96h
Dosing regimen dependent on organisms targeted
Aqueous suspension used
Tested in 5 healthy elephants
Trimethoprim sulfa49
L.a.
22.0
PO, q12h
Tested in 3 elephants
NONSTEROIDAL ANTI-INFLAMMATORIES
Ibuprofen6
E.m.
6.0
PO, q12h
Single dose trial of 10 healthy elephants
Ibuprofen6
L.a.
7.0
PO, q12h
Single dose trial of 10 healthy elephants
Ketoprofen33
E.m.
1.0–2.0
PO, or IV q24 or 48h
Single dose trial of 5 healthy elephants
Phenylbutazone7
E.m
3.0
PO, q48h
Single dose trial of 8 healthy elephants
Phenylbutazone7
L.a.
2.0
PO, q24h
Single dose trial of 10 healthy elephants
OTHER AGENTS
Famiciclovir10
E.m.
8.0–15.0
PO or rectally, q8h
Ivermectin22
L.a.
0.2–0.4
PO
Single dose trial of 6 healthy elephants ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Proboscidea
Chapter 53