2 Principles of cancer surgery
In most cancer patients, obtaining a preoperative diagnosis before contemplating surgery is desirable. Knowledge of the type and possible grade of the tumour will allow the surgeon to answer the following questions:
SURGICAL MARGINS
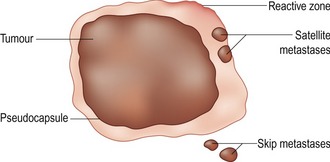
The key to successful surgical cancer management is very much dependent, in the majority of cases, on obtaining margins of normal tissue in addition to the main tumour mass. Even using this approach will not guarantee the complete removal of the tumour as there are often tumour cells that infiltrate the surrounding normal tissue in the form of ‘satellite’ or ‘skip’ metastasis (Fig. 2.1). Therefore in most circumstances there is a greater likelihood of complete local excision when wider margins are taken. The exact distance recommended depends on the tumour type, biological behaviour and anatomical location. For example with low- or intermediate-grade mast cell tumours a margin of 2 cm laterally is recommended and results in the complete excision of the majority of tumours. Deep margins must not be disregarded. However, often tumours lie over naturally resistant anatomical barriers such as fascia, ligaments and tendons which are resistant to tumour spread and therefore if a fascial plane is included in the deep margin this would normally be sufficient as an adequate surgical margin.
There are four basic types of tumour resection depending upon the location of the surgical margin:
SURGICAL TECHNIQUES
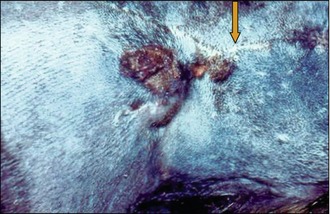
The first attempt at complete excision will always give the best results with locally aggressive and/or malignant tumours. If an excisional biopsy has been previously performed with tumours such as soft tissue sarcomas then the chances of complete excision and therefore a potential cure are reduced. This is because disruption to the tumour from the first surgery can result in tumour seeding to surrounding tissues. Furthermore, disturbance of normal tumour margins can make identification of ‘normal’ versus ‘abnormal’ tissue difficult and also there will be less available local skin for adequate closure. For these reasons a second surgery normally requires even greater margins of excision compared with the first (Fig. 2.2). The exception to this rule is when the tumour type will not affect future treatment options (e.g. mammary tumours, single pulmonary and splenic masses) and in these situations, excisional biopsy is acceptable.
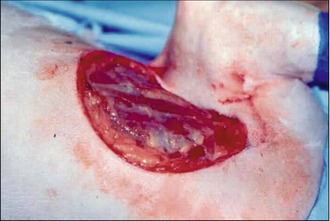
Known malignant tumours should be removed with an adequate margin of normal tissue. Recommendations are that locally aggressive tumours be removed with a minimum of 2 cm margins in the lateral planes and one fascial plane in the deep margin. It is not enough to just ‘shell’ out the tumour and then go back and remove further tissue as this may cause seeding and lead to recurrence. Attempts must be made to avoid disruption to the tumour and perform the excision by cutting through normal, disease-free tissue only (Figs 2.3, 2.4).

Tumours should always be handled carefully and if possible other means of tumour retraction other than using the hand should be used. This can be in the form of stay sutures, Allis tissue forceps or laparotomy sponges (Fig. 2.5). This will help to avoid tumour cell seeding into local, surrounding tissues. Lavage of the excision site with sterile physiological saline before closure may also be utilized to reduce the number of tumour cells remaining in the wound.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


