CHAPTER 170 Prevention of Estrous Behavior in Performance Mares
Veterinarians are often asked by owners to control or eliminate a mare’s estrous behavior. Owners may describe mares as less attentive or less cooperative during estrus so that they do not perform well. For these reasons many owners may prefer to prevent estrous behavior altogether.
PERSISTENT ESTRUS
Persistent estrus is commonly seen in the early spring transitional period and is physiologically a normal phenomenon in the mare. Transitional mares may have irregular periods of estrus or, alternatively, prolonged periods of estrus. The unacceptable behavior associated with this transitional period often subsides once the mare moves into the ovulatory season and estrus cycles become predictable. If the transition period becomes prolonged, hormonal treatments may be beneficial. Treating a transitional mare that has moderate-sized ovarian follicles (greater than 25-mm diameter) with progesterone (Table 170-1) supplementation for 14 days often results in a normal estrus and ovulation following discontinuation of treatment. A transitional mare with one or more follicles larger than 35 mm may respond to ovulation-inducing agents such as deslorelin or human chorionic gonadotropin (Table 170-2). Signs of estrus should cease in 2 or 3 days.
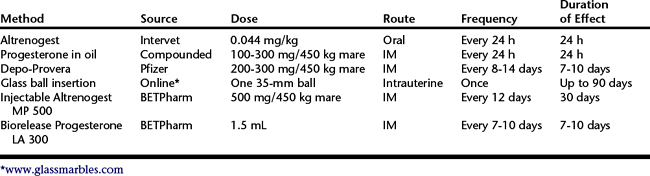
Table 170-2 Drugs, Routes, and Doses of Ovulation-Inducing Agents Used for Estrus Suppression
| Drug | Route | Dose |
|---|---|---|
| Human chorionic gonadotropin (hCG) | IV or IM | 2500 to 3500 international units |
| Deslorelin implant (Ovuplant) | SC | One 2.1-mg implant |
| BioRelease deslorelin (BETPharm) | IM | 1.5 mg |
IM, intramuscular; IV, intravenous; SC, subcutaneous.
PELVIC PAIN DURING ESTRUS
Midcycle pain during ovulation (termed mittelschmerz) is common in women. A similar syndrome of periovulatory pain appears to affect mares. In most mares during estrus, per rectum palpation of a large ovary elicits discomfort. Ovulation is predominantly an inflammatory process, and pain associated with the periovulatory period is common. The events leading to ovulation include a significant increase in ovarian blood flow, connective tissue breakdown, release of inflammatory mediators, and contraction of the ovary. Some mares appear to develop hind limb lameness on the side corresponding to the large growing ovarian follicle. In Standardbred racing mares, the driver may notice that the mare is “on the line” on the corresponding side. Mares performing dressage may be reluctant to bend and engage the hind end or may be resistant to moving freely forward off the rider’s leg. Diagnosis is made by palpation and ultrasound examination of the reproductive tract at the time the mare has signs of pain. A large follicle on a tender ovary on palpation is highly suggestive as the cause of the pain. An ovulation-inducing agent (see Table 170-2) may be given if a follicle with a diameter larger than 33 mm is detected, which usually results in ovulation within 48 hours. The signs of pain usually disappear within a day or two following ovulation. If pain recurs with each cycle, one of the estrus suppression techniques given below may be used to prevent follicular development and ovulation.
Pneumovagina As a Cause of Pelvic Pain
Pneumovagina resulting from poor perineal conformation is common in performance mares. Lean, fit performance mares lack perineal fat, which may result in tipping of the vulva and a predisposition to pneumovagina. Chronic pneumovagina is irritating to the vestibulovaginal mucosa and may induce signs of chronic irritation, including frequent urination, vulvar discharge, and rubbing the tail or perineum. In addition, a characteristic hypersensitivity of the flanks and hindquarters to the touch may be seen. Such mares may uncharacteristically kick out when touched or become increasingly aggressive and agitated. Vaginoscopic examination often reveals vaginitis and cervicitis. Ultrasonography may reveal hyperechoic foci in the uterus, consistent with air contamination. Such mares benefit from placement of a Caslick’s suture in the vulva, with irritation and agitated behavior typically subsiding promptly thereafter.



