CHAPTER 28 Strangles: Immunology and Management
Strangles is an acute, highly contagious disease characterized by fever, inflammation of the upper respiratory tract mucous membranes, purulent nasal discharge, and abscesses of the mandibular and retropharyngeal lymph nodes. The causative organism, Streptococcus equi (subsp equi), is an obligate parasite of equids that rarely infects other hosts. S. equi is a clonal derivative of a Streptococcus zooepidemicus ancestor, shows very little antigenic variation, and stimulates a protective immune response that clears the infection from most horses during convalescence. Infection is maintained by ongoing transmission to susceptible horses and by intermittent shedding from occasional carrier horses with unilateral or bilateral guttural pouch empyema. Most outbreaks begin following introduction of a horse incubating the disease or that has recently recovered but not cleared the infection. S. equi-free status is eventually attained in most herds following a strangles outbreak, so many horse farms, geographic areas, and countries (such as Argentina, Japan, and Ireland) have enjoyed strangles-free status for long periods during the past century.
IMMUNOLOGY OF STRANGLES
Immune Response
Infection generates an acquired immune response that is protective in approximately 75% of horses for up to 5 years. Foals of previously infected mares may be immune for 3 to 4 months. Convalescent serum and mucosal antibody responses are targeted at more than 20 surface exposed and secreted proteins of S. equi. Antibodies against SeM (M-like protein) are opsonizing, antibodies against the pyrogenic exotoxins neutralize pyrogenicity, and mucosal IgA antibodies specific for tonsil-binding proteins may block adhesion. IgGb is the predominant SeM-specific immunoglobulin isotype in both acute and convalescent sera. Significant increases in this isotype and of IgGa are detectable within 2 weeks after co-mingling exposure to an infected horse. IgG(T)-specific antibody appears a week or two later. Concentrations of antibody against SeM and other immunoreactive proteins of S. equi peak about 5 weeks after exposure and slowly decline over the following 6 months to levels slightly above those at time of initial infection. Nasal mucosal IgA peaks at about 6 weeks, a week or two after mucosal IgGb, and declines at a rate similar to that of specific serum IgGb.
Vaccines
The first reported use of strangles vaccine dates from the late 1700s, when Richard Ford, an English veterinarian, practiced a technique that resembled smallpox vaccination whereby the inside of the lip was abraded and rubbed with lint impregnated with pus from a strangles abscess. The resulting infection spread to local lymph nodes, inducing systemic resistance to natural infection. Much later, French military veterinarians used a serum-vaccine approach whereby inoculation of hyperimmune serum was followed by subcutaneous inoculation of a culture of live S. equi. Although these procedures were reputed to elicit a high level of protective immunity, they did not become popular because of the frequent occurrence of abscesses at inoculation sites. Nevertheless, they provided evidence that preparations of live S. equi could serve as effective vaccines (Table 28-1).
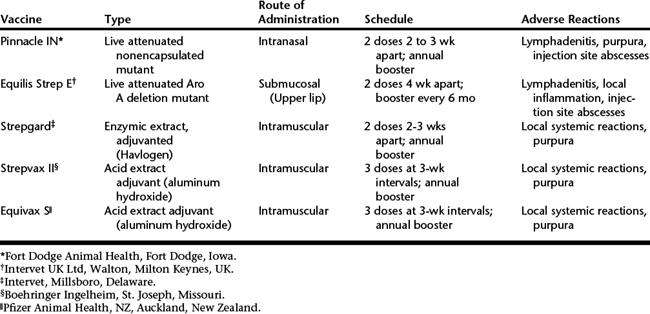
Extract Vaccines
Immunogenic proteins of S. equi, including SeM extracted by hot acid or mutanolysin plus detergent and adsorbed to aluminum hydroxide, have been widely used as strangles vaccines in North America and have proved highly potent with respect to SeM-specific serum IgGb, but not mucosal IgA, antibody responses. These vaccines are inoculated intramuscularly or subcutaneously and elicit serum antibody responses 7 to 10 days later. Responses are Th2 cytokine-driven, with dominance of SeM specific serum IgGb and IgG(T). Mucosal IgA or cell-mediated immune responses of value in intracellular killing of S. equi in tonsillar follicular tissue are not elicited. Naïve horses and foals require two or three doses at an interval of 2 weeks followed by annual booster doses. Colostral levels of antibody are boosted by prepartum vaccination of mares a month before expected date of foaling.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


