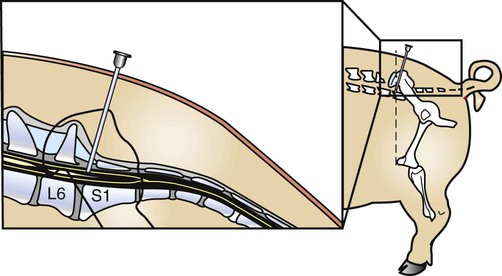
After reading this chapter, you will be able to • Prepare the surgical patient for surgery • Perform local anesthesia or assist the veterinarian in administering local anesthesia • Assist or perform induction and maintenance of anesthesia • Provide anesthetic monitoring • Manage patient recovery and immediate postoperative care • Discuss the basic risks and possible complications associated with anesthesia and surgery The proper site for the epidural must be identified. The lumbosacral junction is just caudal to a line drawn transversely through the animal to connect the crests of the wings of the ilium, where the line bisects the dorsal midline. In small swine, the wings of the ilium are palpable. In large swine, anatomical landmarks must be relied upon to locate the site. Large swine are preferably injected in the standing position, standing squarely on all four legs. Looking at the pig from the side, a vertical line is drawn upward from the patella; this line usually identifies the cranial extent of the crest of the ilium. The needle is inserted 1 to Before administering anesthesia to swine, the following risks should be considered. • The larynx of swine is sensitive to physical stimulation. Pressure and touch, even from accumulated saliva, can trigger a laryngospasm. • The laryngeal lumen of the pig is small in relation to the size of the animal. A pig weighing 100 kg requires an endotracheal tube that would fit a large dog (≈14-mm internal diameter). Flexing the neck partially occludes the laryngeal entrance. Salivation, which is common in anesthetized pigs, can result in accumulations of saliva in the pharynx and laryngeal entrance that actually occlude the larynx. • Laryngeal edema results readily in swine due to their relatively fragile laryngeal mucosa. The laryngeal mucosa is quite easy to traumatize during endotracheal intubation and responds quickly with swelling. This edema of the larynx causes further narrowing of the already small lumen diameter. Various anesthetic induction and maintenance regimens are available for swine. Withdrawal times for meat-producing animals should be observed. A quiet induction area is preferred. Restraint in a chute or crate is generally less stressful than other forms of physical restraint (e.g., snout restraint). Some of the techniques in use are listed in Box 24-1. BOX 24-1 Anesthetic Induction and Maintenance Regimens Available for Swine • Telazol/ketamine/xylazine (TKX): All three drugs are mixed together in the Telazol vial and given intramuscularly (IM). This popular combination provides short-term anesthesia (20–30 minutes). It also can be used for stages from induction to inhalant gas maintenance. Endotracheal intubation can be performed with this combination. Repeated injections of the combination can be used to extend the length of general anesthesia. Recovery from anesthesia occurs in 60 to 90 minutes. • Atropine/acepromazine/ketamine: Atropine and acepromazine are given IM, followed by ketamine IM approximately 20 minutes later. This combination is useful for minor, short procedures. Anesthesia lasts approximately 10 to 15 minutes. Analgesia must be supplemented with local anesthetics for painful procedures. • Atropine/xylazine/ketamine: Atropine and xylazine are given IM, followed by ketamine IM approximately 10 minutes later. Anesthesia lasts about 10 to 15 minutes. • Xylazine/Telazol: Xylazine is given IM, followed by Telazol IM 5 minutes later. Although analgesia and muscle relaxation are good, the depth of surgical anesthesia may be light and of short duration. Drowsiness after recovery may be prolonged (up to 24 hours). • Intratesticular sodium pentobarbital: A technique for anesthesia for castration of large boars has been described. Sodium pentobarbital is injected into each testicle to produce anesthesia in approximately 5 minutes. Removal of the testicles effectively removes the source of the anesthesia. • Inhalant gases: Mask induction, with or without prior sedation, can be used in small or heavily sedated swine. Halothane, isoflurane, and sevoflurane all are suitable for use in swine, but halothane is generally avoided because of the risk of inducing malignant hyperthermia in susceptible families of swine. • Intravenous thiobarbiturates: An intravenous catheter or butterfly administration set can be used in the ear vein to inject thiobarbiturates. This may be the safest choice for anesthesia in pigs from family lines susceptible to malignant hyperthermia.
Porcine Surgical Procedures
Swine Surgery and Anesthesia
Local Anesthesia
Lumbosacral Epidural Anesthesia
 inches caudal to this line, on dorsal midline (Fig. 24-1).
inches caudal to this line, on dorsal midline (Fig. 24-1).
General Anesthesia
Anesthetic Risks for Swine
Swine Are Prone to Hypoventilation
Airway obstruction
Preanesthetic Preparation and Anesthetic Management
Induction Drugs
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


