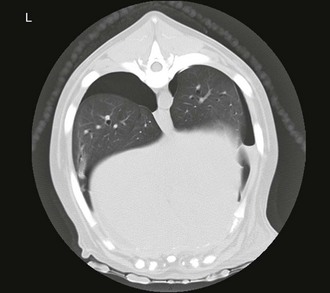
Chapter 165 Pneumothorax is defined as free air in the pleural space. Normal intrapleural pressure is approximately −5 cm H2O, which means that, in the healthy dog or cat, intrapleural pressure is negative compared with the atmosphere. This negative intrathoracic pressure helps to maintain lung expansion and promote venous return. Normal intrapleural pressure varies depending on the phase of respiration, with inspiration associated with more negative pressure during spontaneous breathing. Pneumothorax develops when there is either leakage of air from damaged or diseased pulmonary parenchyma or external damage to the thoracic cavity resulting in the entrance of air into the chest cavity from the atmosphere. Clinical signs of pneumothorax include a short and shallow (“restrictive”) breathing pattern and absent lung sounds on thoracic auscultation. Diagnosis of pneumothorax may be confirmed with thoracic radiographs (Figure 165-1) or by a positive thoracocentesis. Computed tomography (CT) will also highlight pneumothorax (Figure 165-2). In emergency practice, limited ultrasonography of the thoracic cavity (thoracic focused assessment with sonography for trauma [T-FAST]) also has been used to detect pneumothorax in dogs and cats with suspected traumatic pneumothorax (Lisciandro, 2008). Pneumothorax can be characterized as traumatic, spontaneous, or iatrogenic, and as open or closed (Pawloski and Broaddus, 2010). A tension pneumothorax can result from any type of pneumothorax, although it is usually closed. It is characterized by a barrel-shaped (hyperinflated) appearance to the chest cavity with limited thoracic motion despite vigorous movements of the head and neck in an attempt to ventilate, and by hypoxemia and cardiovascular collapse caused by continued entrapment of air within the pleural space due to lack of an escape pathway. Figure 165-1 Lateral thoracic radiograph documenting pneumothorax in a dog. Note apparent “lifting” of the heart off of the sternum and retraction of the dorsal lung fields. Figure 165-2 Computed tomographic image of spontaneous pneumothorax in a dog showing retraction of the lung from the rib cage on the left and pleural air accumulation. Heimlich valves are one-way valve devices that attach to large-bore thoracostomy tubes. They are used very commonly in people and large animals such as horses. In cats and in dogs weighing less than 20 kg Heimlich valves are potentially less effective because of limited intrathoracic pressure changes. However, a recent report describes successful use of Heimlich valves in 34 dogs (Salci et al, 2009), and their use should be considered, particularly when continuous-suction units are not available. Each Heimlich valve costs approximately $30 USD. A potential problem with valves is that blood or other fluid sometimes can collect in the valve. This can lead to clogging and malfunction of the device. Patients with Heimlich values should be closely monitored.
Pneumothorax

Therapeutic Options for Treatment of Pneumothorax
Heimlich Valves
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


