CHAPTER 63 Pleuropneumonia
Pleuropneumonia typically develops following bacterial colonization of the lower respiratory tract and extension to the pleural space. Bacterial colonization occurs when pulmonary defense mechanisms are compromised (especially the mucociliary clearance mechanism). This disease is common in any horses that are transported long distances. Thoroughbreds and Standardbreds are more predisposed to developing pleuropneumonia than other breeds, possibly because they are shipped more frequently and for longer distances than horses of other breeds with more comingling with other horses. Forty percent of horses with pleuropneumonia have a history of transport within the 3 weeks preceding development of clinical signs. As few as 12 hours of confinement with the head elevated is enough to increase purulent secretions and bacterial numbers in the lower respiratory tract through compromised mucociliary clearance. Twelve hours without head restraint are required after confinement to restore normal mucociliary clearance. Horses transported without head restraint do not have increases in inflammatory cell numbers or bacterial numbers in the lower respiratory tract, implying that decreased mucociliary clearance from head restraint is more important than the other stresses of transport in development of pleuropneumonia.
CLINICAL SIGNS AND DIAGNOSIS
Ultrasonographic Examination
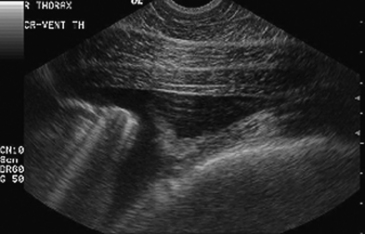
Ultrasonographic examination is the most sensitive diagnostic and monitoring tool for detecting pleuropneumonia. In the healthy horse, only the body wall and parietal pleura can be assessed with ultrasound. In the horse with pleuropneumonia, the dorsal extent of fluid accumulation, depth and echogenicity of fluid, visceral pleura, underlying consolidated lung, and superficial pulmonary abscesses can be identified (Figures 63-1 and 63-2).
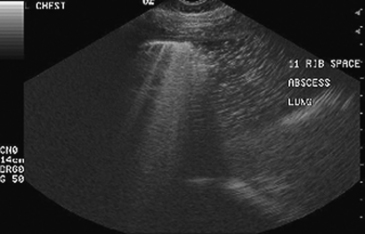
Figure 63-1 Sonographic appearance of pleural abscess and aerated lung in a horse with pleuropneumonia.