Parturition and Obstetrics
Dystocia is without doubt the most common emergency in camelid practice and has been recognized as one of the leading causes of mortality and reproductive losses.1,2 Prompt diagnosis and management of obstetric situations is critical for the survival of the newborn as well as for the prevention of further complications that could be life threatening or end the reproductive function in the female. Although many of the examination techniques and obstetric procedures used in camelids are similar to those used in other large animal species, a few peculiarities do exist for camelids that the practitioner should be aware of. This chapter described the normal parturition process and approach to dystocia in alpacas and llamas.
Normal Parturition (Eutocia)
Pregnancy Length and Premonitory Signs of Parturition
Pregnancy length in llamas and alpacas has traditionally been reported to be 340 ± 5 days (335 to 359 days). However, data from outside South American countries show a great variability in the duration of pregnancy, ranging from 320 to 400 days (Figure 24-1).2
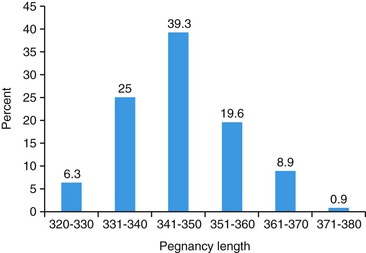
Figure 24-1 Distribution of pregnancy length in an alpaca herd in the United States (n = 113). (Adapted from Tibary A, et al.: Management of dystocia in camelids. In Proceedings of the 41st Annual Convention of American Association of Bovine Practitioners, Charlotte, NC 2008 pp. 166-176.)
Factors suspected to affect pregnancy length include breed, sex of the fetus, season, nutrition, and sire and dam effects. In alpacas, pregnancy length is, on average, 12.5 days longer in spring-mated alpacas than in fall-mated alpacas. Breeders in North America reported unusually longer pregnancy lengths in years with longer and colder winters.3
Mammary gland development occurs during the last month of pregnancy. Multiparous females may show obvious udder enlargement within the last 2 weeks before parturition. Primiparous females may not show significant udder development until a few days after parturition. Excessive mammary edema extending cranially to the xyphoid area may be seen in some females. Other females may show ventral edema, swelling of the teats, and waxing a week before parturition. Colostrum is detected 6 days and 4 days before parturition in pluriparous and primiparous animals, respectively.4 Electrolyte analysis in mammary gland secretions does not provide a good indication of parturition as it does in the equine. However, in cases where induction of parturition is considered, the presence of thick sticky colostrum is correlated with a very good outcome for the cria.
Stages of Parturition
Parturition in camelids is a relatively short event compared with that in ruminants.2 Preparation of the preparturient female is an important step to avoid puerperal problems for the dam or sickness in crias. It is important to maintain clean and dry stalls or paddocks that are provided with fresh water and good quality hay and to minimize any stressful or uncomfortable situation for the animal.
The tail of the female may be wrapped as soon as dilation of the vulva is noticed. The tail bandage should not be too tight and should be checked daily and changed every other day to avoid damage to the tail. In South American conditions, most of the births (93.5%) occur between 7:00 A.M. and 1:00 P.M., and none is observed at night.5,6 This is probably an adaptation feature in these animals to ensure the birth of the young (cria) in the most favorable time of the day for ambient temperatures and protection against predators. In North American rearing conditions, parturition may be observed at other times of the day.
As for all other species, stages of parturition are traditionally divided into three stages. The first stage of labor, or the preparatory stage, varies greatly in duration and may be as short as 3 hours and up to 48 hours long. This wide range in duration of the first stage of labor may be a result of environmental as well as individual factors. The female shows increased restlessness and anxiety and usually isolates itself from the rest of the herd. Appetite is often decreased; however, some multiparous females will maintain normal appetite throughout parturition. During this stage, an increased frequency of defecation and urination (increased visits to the “dung pile”) is observed. The female shows signs of mild discomfort and frequently alternates between the standing and sitting positions or walks in circles (Figure 24-2). These signs intensify with the progressive stretching and dilation of the cervix from the pressure exerted by the fetus as a result of uterine contraction. Abdominal contractions and straining becomes more frequent (one contraction every 2 minutes) toward the end of the first stage. Some females may go off feed and show signs of colic. Excessive signs of rolling, kicking at the belly, and vocalization or grunting should be taken seriously, as they may signal an abnormal situation such as in the case of uterine torsion.

Figure 24-2 Stage 1 of labor: Increased defecation and urination. (Photo courtesy of Dale and Leslee Miller.)
The second stage of labor starts with the rupture of the chorioallantoic sac (allantochorion) and ends with the complete expulsion of the cria. It is very short in duration and is completed within 20 minutes on average (range 5 to 30 minutes), being longer in duration in primiparous females (up to 80 minutes). Nearly all crias are born in an anterior longitudinal presentation and in the dorsosacral position, with the chin resting on the carpus. The amniotic sac appears at the vulva within 2 or 5 minutes of the rupture of the allantochorion (Figure 24-3).7 At this stage, the head of the cria can be easily palpated within the pelvic canal. As uterine and abdominal contractions increase in intensity and frequency, the nose appears first at the vulva, followed by one foreleg.7 The other foreleg appears 3 to 5 minutes after the rupture of the amniotic sac. In some situations, the head may be completely exteriorized before both feet appear (Figure 24-4). The forelegs are extended either above or below the head at this stage. The head and forelegs up to the carpal joints should be out within 5 to 10 minutes of rupture of the amniotic sac.2,7 The female may stand at this stage, with the head, neck, and forelegs of the fetus exteriorized (Figure 24-5). Most (65% to 73%) of the fetuses are delivered while the dam is standing. Powerful abdominal contractions are needed to push the fetus out at the level of the shoulders and thorax. The frequency and intensity of uterine and abdominal contractions are increased with the passage of the fetus through the cervical canal (Ferguson reflex). Some females may lie down on the side during this stage and help orient the fetus to a diagonal (dorsoilial) position to take advantage of the widest diameter of the pelvis. The umbilical cord ruptures soon after birth about 3 to 10 cm from the fetal abdominal wall. A twisted portion of 10 to 20 cm is seen hanging from the vulva of the dam. The dam turns immediately to smell the newborn, but licking is not common in camelids.2,7

Figure 24-3 Stage 2 of labor: Appearance of the amniotic sac (“second water bag”) and nose of the fetus. (Photo courtesy of Dale and Leslee Miller.)


Figure 24-5 Stage 2 of labor: Delivery of the front legs. (Photo courtesy of Dale and Leslee Miller.)
Inspection of the fetal membranes is very important and should be performed, whenever possible, to detect any abnormality such as placentitis and to evaluate the presence of both uterine tips to ensure that the placenta is not retained partially. In alpacas, the placenta weighs between 0.8 to 1 kg. The chorionic surface usually has a dark red (burgundy) color and a velvety aspect because of the presence of microvilli. The placenta may show areas with reduced microvilli along the bifurcation and at the tip of the horns. Although not always present, hippomanes (one or two) may be found in the allantoic sac of the camelid.2
Induction of Parturition
Induction of parturition may be indicated when the dam’s health is in jeopardy or if the fetus is showing obvious signs of distress. Induction of parturition should not be attempted unless uterine torsion is ruled out. Induction of labor is not a management procedure and should not be used as such. Each case should be carefully studied. The best chances for a good outcome for the neonate (reduce the risk of neonatal maladjustment syndrome) is to induce only when breeding dates are known precisely, the stage of pregnancy is adequate (minimum 330 days), and colostrum secretion in the mammary gland is apparent. Development of the mammary gland and presence of thick colostrum is, in our opinion, the most important criterion for induction. Because camelids rely primarily on progesterone from the corpus luteum (CL) to maintain pregnancy, induction is easily achieved by administration of a luteolytic dose of prostaglandin F2-alpha (PGF2α; dinoprost tromethamine, 5 milligrams [mg], intramuscularly [IM]) or its analogue cloprostenol (250 micrograms [mcg], IM). Caution should be exercised when using dinoprost because it may cause severe respiratory distress and pulmonary edema in compromised females. Oxytocin and dexamethosone should not be used for induction of parturition in camelids, as these agents are not efficacious. Dexamethasone treatment results in intrauterine fetal death.4 In one study, the mean time from treatment with fluprostenol (40 mcg, IM) to parturition was 21 hours and 29 minutes (range 19 to 29 hours).4 In our experience, in emergency induction of parturition, the interval from cloprostenol injection to parturition is 20 hours, on average, but ranged from 8 to 30 hours. In our protocol for the management of high-risk pregnancies, the fetus is evaluated at 12 hours and at 20 hours after treatment, and if the fetus shows signs of distress (persistent tachycardia >130 beats per minute [beats/min], or bradycardia <50 beats/min) or is not delivered by 24 hours after induction, a cesarean section is performed.
Incidence and Causes of Dystocia
Dystocia is relatively uncommon in alpacas and llamas, with fewer than 5% of birthings requiring assistance.1,2 The incidence of dystocia in camelids has been estimated to be between 2% and 5% of all births.2,8 In our practice, dystocia requiring major obstetric intervention represents less than 1% of all births (A. Tibary, personal observation). Early diagnosis of dystocia is very important because it may evolve rapidly to a critical situation endangering the life of both the fetus and the dam.
Dystocia of maternal origin may be caused by uterine inertia, small pelvic size, failure of cervical dilation, and uterine torsion. Failure of cervical dilation and uterine torsion are the most common causes of dystocia of maternal origin.2,8,9 Failure of cervical dilation is associated with long-term progesterone supplementation during pregnancy.7
Approach to Dystocia in Camelids
Clinical Evaluation of the Dam
Sedation may be needed in some cases to complete the evaluation. Choices of drugs and dosage for sedation should take into account their effects on the fetus. Butorphanol tartrate (0.05–0.1 milligram per kilogram [mg/kg]) provides good sedation and has minimal effect on the cardiovascular system.10 However, a mild decrease in systemic vascular resistance, which may be of consequence if the blood flow to the uterus is already restricted, has been observed. Epidural analgesia may be needed for evaluation per vaginum or per rectum. An 18-gauge, 1.5-inch needle is placed on the dorsal midline, with the bevel facing cranially and at a 60-degree angle to the tail head. The duration of analgesia depends on the drug used. In the case of lidocaine (0.2 mg/kg, maximum 1 mL/45–50 kg, maximum of 2 mL for the alpaca and 2.5 mL for the llama), onset of analgesia is seen 5 minutes after administration and lasts about 1 hour to 1.5 hours. Administration of xylazine (0.1 mg/kg) provides up to 3 hours of anesthesia, and the combination of xylazine and lidocaine (xylazine 0.17 mg/kg; lidocaine 0.22 mg/kg) provides up to 6 hours of analgesia.1
The quantity and quality of fecal material within the rectal cavity should be evaluated prior to transrectal palpation. Diarrhea is often seen in severely distressed animals. Absence of fecal material, presence of mucoid content, or both may be caused by intestinal transit disorders or tenesmus. Infusion of a mixture of 10 mL of 2% lidocaine in 60 to 100 mL of lubricant in the rectal cavity provides some rectal relaxation and reduces straining. It is important, however, to keep the use of lidocaine to a minimum to avoid toxicity in case a cesarean section is needed. The toxic dose of lidocaine has not been determined for alpacas and llamas, but most practitioners tread on the safe side and use 4 mg/kg as the maximum dose. The primary objective of transrectal palpation is to determine the location and direction of the broad ligaments and evaluate the caudal abdomen for any masses or abnormalities of the pelvic area, kidneys, and bladder. Transrectal palpation in the female sitting in the sternal position may offer some challenges to the inexperienced practitioner.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


