Chapter 21 Pacemaker Therapy
PRE-IMPLANTATION EVALUATION
• After confirming that an indication for permanent cardiac pacing exists, the most appropriate pacing system and pacing mode for the patient should be determined. Factors to be considered for this determination include: (1) specific underlying rhythm disturbance, (2) overall physical condition, (3) nature of any associated medical problems, and (4) exercise requirements of the patient.
COMPONENTS AND TYPES OF PACING SYSTEMS
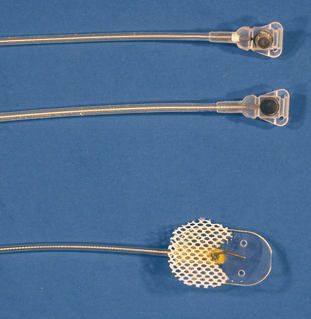
• Permanent transvenous pacing leads use either active or passive fixation for attachment of the lead tip to the endomyocardium. A passive fixation transvenous lead has a “collar” of tines encircling the distal tip which anchor the lead by becoming enmeshed in the right ventricular trabeculae (Figure 21-1). An active fixation lead has a small metal helix that exits the tip of the lead to penetrate the endomyocardium (see Figure 21-1). Although the type of fixation of a transvenous lead does not appear to affect the incidence of lead dislodgement, it is wise to avoid use of passive fixation in animals with significant right ventricular dilation.
• Another consideration for selection of the pacing system is whether a unipolar or bipolar system is desired. A unipolar pacing system uses the lead tip as the cathode (negative pole) of the electrical circuit and the metal case of the pulse generator as the anode (positive pole). The impulse travels from generator to myocardium via the lead and returns to the generator via the soft tissues. A major disadvantage of unipolar pacing is the proximity of the electrical circuit to skeletal muscle which may result in skeletal muscle twitching. Advantages of unipolar pacing include smaller diameter of the pacing lead, a single attachment site of the lead to the epicardium when epicardial pacing is used, and superior sensing of endogenous cardiac potentials. Bipolar pacing systems have two closely spaced electrodes located distally on a transvenous lead or closely adjacent at two ends of an epicardial lead (Figure 21-2). One electrode (usually the distal electrode on a transvenous bipolar lead) is the cathode, and the other is the anode. Electrical impulses travel to the cathode from the pulse generator and return to the anode to complete the circuit. In the majority of cases a bipolar pacing system is preferred because there is less potential for electromagnetic interference (EMI) with bipolar pacing and because of absence of skeletal muscle stimulation.

Single- vs. Dual-Chamber Pacing
• Although AV synchrony may not be clinically important for many dogs and cats needing chronotropic support, pacing that provides AV synchrony will provide higher systemic pressure and lower ventricular filling pressures than single-chamber ventricular pacing. Therefore, dual-chamber pacing to provide AV synchrony is likely to be important in animals with underlying structural heart disease or in working animals such as military dogs and agility dogs.
Pacemaker Nomenclature
• Pacing nomenclature was established in 1974 and updated in 2002 for use in human medicine. This nomenclature also applies to veterinary pacemaker therapy, and awareness of the nomenclature is important for understanding cardiac pacing. Pacing nomenclature classifies pacing based on the site and mode of both pacing and sensing using a series of three to five letters (Table 21-1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


