Chapter 2 Radiology of the Heart
RADIOGRAPHIC TECHNIQUE
Exposure Technique and Film Quality
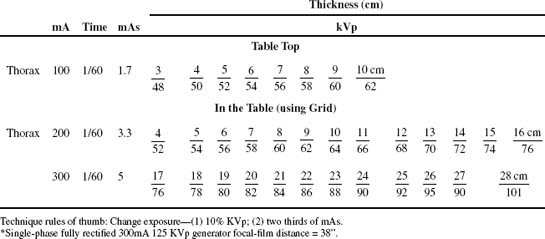
Radiographic Projections
Lateral Projection
Guidelines for proper exposure and positioning of a lateral thoracic radiograph (Figure 2-1) include:
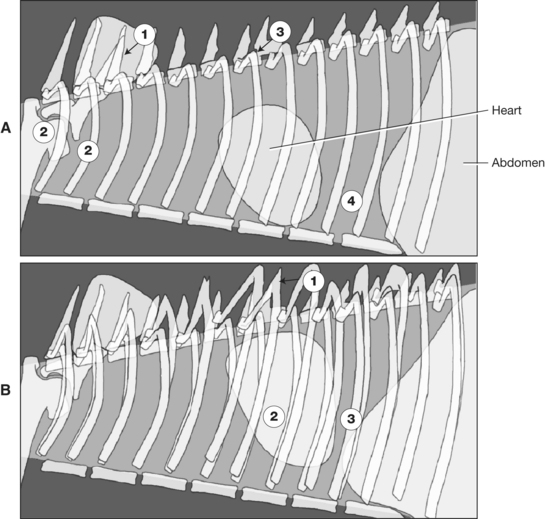
Figure 2-1 A, Guidelines for proper exposure and positioning of a lateral thoracic radiographic projection. (1) Exposure should allow delineation of the thoracic vertebral dorsal spinous process superimposed over the scapula. (2) The forelimbs should be pulled forward to provide an unsuperimposed view of the cranial thorax. (3) The dorsal rib heads should be superimposed (compare with B). (4) The exposure should be performed during inspiration, which provides maximum separation between caudal cardiac margin and diaphragmatic cupula. B, Improperly positioned lateral thoracic radiographic projection (compare with A). (1) Nonsuperimposed left and right rib heads. (2) The oblique projection markedly distorts cardiac silhouette conformation and intrathoracic position. (3) Expiratory phase radiographic exposure with poor lung volume between caudal cardiac margin and cupula of the diaphragm.
PROJECTION SELECTION IN CARDIAC-RELATED PATHOLOGY
Pulmonary Edema
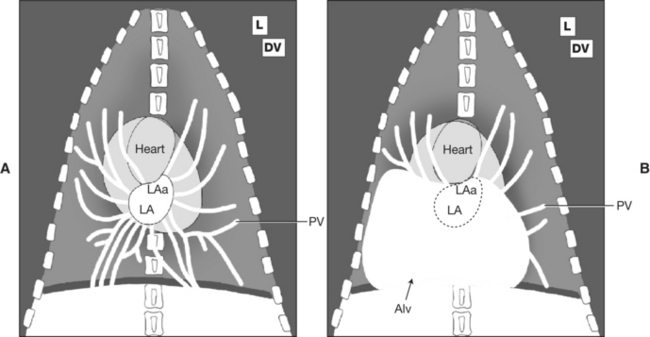
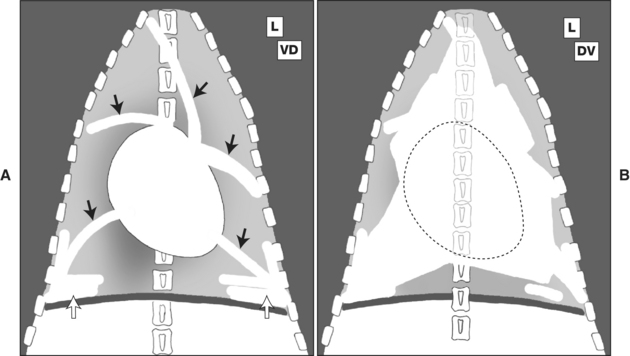
Figure 2-3 A, Normal radiographic definition and contrast of pulmonary venous vasculature (PV) with surrounding normal radiolucent lung parenchyma. L, Lateral; DV, dorsoventral; LA, left atrium; LAa, left atrial auricular appendage. B, Radiographic obliteration of pulmonary venous vasculature (PV) by alveolar consolidation (Alv) of hilar and caudal lung lobes, a characteristic distribution for cardiogenic pulmonary edema.
Pleural Effusion
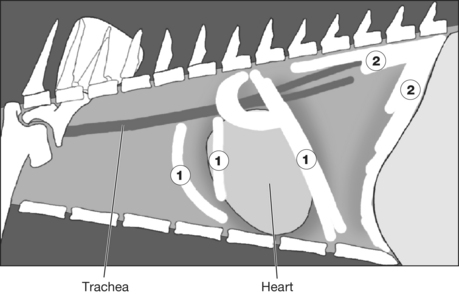
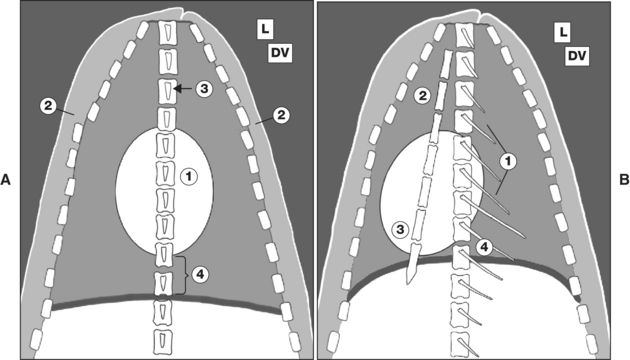
Figure 2-4 Lateral thoracic radiographic projection of pleural effusion. Intrathoracic fluid accumulation causes separation of adjacent lung lobes by (1) linear interlobar opacities, radiographically defined as pleural fissures, and (2) separation of lung lobes from the thoracic wall.
RADIOGRAPHIC ANATOMY
Lateral Thoracic Radiographic Projection
Cardiac Parameters
Even though the lateral radiographic projection defines the cranial-caudal and dorsal-ventral dimensions of the thorax, the anatomy of the heart of the dog and the cat as it resides in the thorax also allows this projection to detail the left and right aspects of the heart. This is because in the dog and the cat the heart is slightly rotated along its base-apex axis, such that the right cardiac chambers are positioned more cranially and the left chambers positioned more caudally. Thus, the cardiac silhouette as it appears on the lateral projection defines the right side of the heart along the cranial margin and the left side is defined by its caudal margin (Figures 2-6 to 2-8).
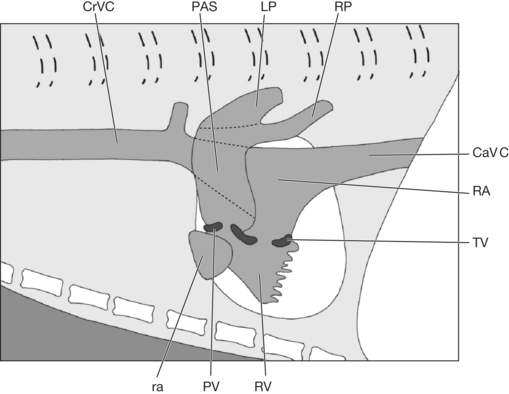
Figure 2-6 Schematic lateral thoracic radiographic projection of the relative position and size of the right-side structures of the heart. Note the more cranial position of the right chambers of the heart. CrVC, Cranial vena cava; PAS, main pulmonary artery; PV, pulmonic valve; ra, right atrial auricular appendage; RV, right ventricle; RA, right atrium; LP, left pulmonary artery; RP, right pulmonary artery; TV, tricuspid valve; CaVC, caudal vena cava.
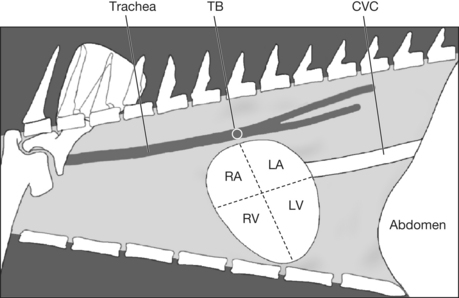
The canine and feline heart shape or radiographic silhouette is ovoid, with the apex more pointed in conformation than the broader base. This base-apex difference in conformation is accentuated in the cat. The heart axis is defined by drawing a line from the tracheal bifurcation (carina) to the apex at an angle approximately 45 degrees to the sternal vertebrae. This angle can decrease in the cat with age and is often called a “lazy” heart. It has been postulated that this may be related to a loss of aortic connective tissue elasticity. This is most often seen in cats older than 7 years. Shallow, barrel-chested dog breeds (Dachshund, Lhasa Apso, Bulldog) tend to have more globular-shaped hearts, with increased sternal contact of the cranial margin of the heart. The heart chambers can be roughly defined by a line connecting the apex to the tracheal bifurcation and a second line perpendicular to the base-apex axis and positioned at the level of the ventral aspect of the caudal vena cava (see Figure 2-8).
The dorsal cardiac margin includes both atria, pulmonary arteries and veins, the cranial and caudal vena cavae, and the aortic arch (see Figures 2-6 to 2-8). The cranial border is formed by both the right ventricle and the right atrial appendage, resulting in the radiographically defined “cranial waist” (see Figures 2-6 and 2-8). The caudal margin is formed by the left atrium and left ventricle, with the atrioventricular junction defined as the radiographic “caudal waist.”
A more objective determination of cardiac size has been formulated for the dog and uses a vertebral scale system in which cardiac dimensions are scaled against the length of specific thoracic vertebrae (Figure 2-9). In lateral radiographs the long axis of the heart (L) is measured with a caliper extending from the ventral aspect of the left main stem bronchus (tracheal bifurcation hilus, carina) to the left ventricular apex. The caliper is repositioned along the vertebral column beginning at the cranial edge of the fourth thoracic vertebra. The length of the heart is recorded as the number of vertebrae caudal to that point and estimated to the nearest tenth of a vertebra. The maximum perpendicular short axis (S) is measured in the same manner beginning at the fourth thoracic vertebra. If obvious left atrial enlargement is present, the short axis measurement is made at the ventral juncture of left atrial and caudal vena caval silhouettes.
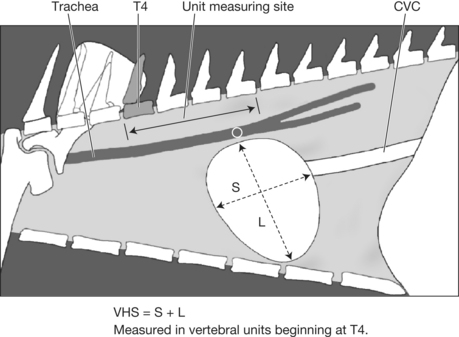
The lengths in vertebrae (v) of the long and short axes are then added to obtain a vertebral heart sum (VHS), which provides a single number representing heart size proportionate to the size of the dog. The average VHS in the dog is 9.7 v (range 8.5 to 10.5 v). Caution must be exercised in some breeds that have excessively disproportionate skeletal–body weight conformations. An example is the English Bulldog, which has relatively small thoracic vertebrae and commonly has hemivertebrae as well; thus, a normal heart may be interpreted as large with the VHS method. Although the VHS concept is more precise, clinical judgment is still necessary to avoid over diagnosing or under diagnosing heart disease.
Vessel Parameters
The main pulmonary artery (pulmonary trunk) cannot be seen on the lateral projection owing to a positive-silhouette sign with the craniodorsal base of the heart. The left pulmonary artery can sometimes be seen extending dorsal and caudal to the tracheal bifurcation (carina). The right pulmonary artery is frequently seen end-on as it leaves the main pulmonary artery immediately ventral to the carina (Figure 2-10). This end-on appearance may be confused with a mass lesion on normal radiographs and is accentuated in cases of pulmonary hypertension such as heartworm disease. The pulmonary veins are best identified as they enter the left atrium caudal to the heart base.
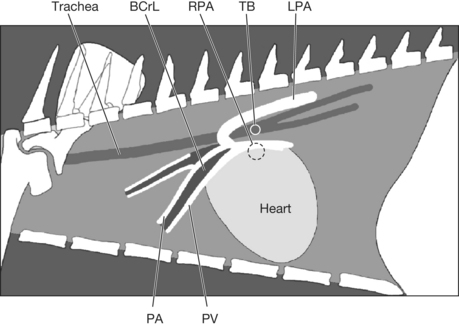
Using the larger, more proximal segments of the mainstem bronchi as a reference, the pulmonary arteries are dorsal to the bronchus, and the pulmonary veins are ventral to the bronchus (see Figure 2-10).
Dorsoventral and Ventrodorsal Projections
Cardiac Parameters
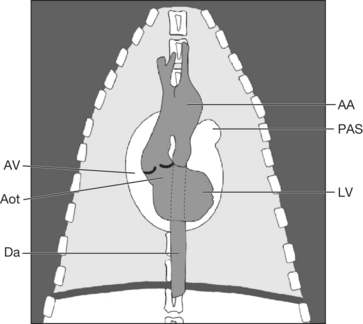
The canine heart appears radiographically as an elliptical opacity with its base-apex axis orientation approximately 30 degrees to the left of the midline. The width of the heart across its widest point is usually 60% to 65% of the thoracic width at its location within the thorax. In the cat the cardiac axis is most commonly on or close to midline, and its width does not usually exceed 50% of the width of the thoracic cavity during full inspiration. The cardiac silhouette may be artificially increased in the obese patient owing to an excessive amount of pericardial fat. In these cases, the cardiac silhouette margin appears to be less well defined or blurred because the margin of contrast between soft tissue (heart), fat (pericardial), and air is not as distinct as that between soft tissue and air.
The margins of the heart that create the cardiac silhouette contain a number of structures that often overlap. A clock face analogy can be used to simplify the location of these structures. The aortic arch extends from the 11 o’clock to 1 o’clock position (Figure 2-11). The main pulmonary artery is located from the 1 to 2 o’clock position, with its radiographic designation as the pulmonary artery segment (PAS) (Figures 2-12 and 2-13). In the cat, the body of the left atrium proper forms the 2 to 3 o’clock position of the cardiac silhouette. In the dog, the left atrium is superimposed over the caudal portion of the cardiac silhouette in the DV projection (see Figure 2-12). With severe cases of left atrial enlargement in the dog, the left auricular appendage contributes to the definition and enlargement of the cardiac silhouette at the 2 to 3 o’clock position (Figure 2-13). The left ventricle forms the left heart margin from the 2 to 6 o’clock position (see Figure 2-11). The right ventricle is located from the 7 to 11 o’clock position (the right ventricle does not extend to the apex of the heart) (Figure 2-14). The right atrium is located at the 9 to 11 o’clock position (see Figure 2-14). Pericardial fat in the dog can asymmetrically contribute to cardiac silhouette enlargement at the 4 to 5 o’clock and 8 to 11 o’clock positions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


