CHAPTER 139 Ocular Squamous Cell Carcinoma
Tumors affecting the orbit, eyelid, or globe often manifest initially as signs of ocular discomfort or mucopurulent discharge, but they can be identified before the development of serious ophthalmic abnormalities through careful ophthalmic examination. Squamous cell carcinoma (SCC) is the most common neoplasm of the equine eye and ocular adnexa and is the second most common tumor affecting the horse overall. SCC may involve any or all of the corneoconjunctiva, bulbar conjunctiva, third eyelid, and eyelids. The biological behavior of SCC varies depending on location, and tumors are typically locally invasive and slow to metastasize. Metastasis to local lymph nodes, salivary glands, and into the thorax can occur. A poorer prognosis has been associated with SCC involving the eyelid, compared with SCC of the nictitating membrane, nasal canthus, or limbus.
EXAMINATION AND DIAGNOSTIC PROCEDURES
The horse should be examined first from a distance to facilitate assessment of facial symmetry and eyelash positioning. One of the first clinical signs observed with ocular pain in horses is ventral deviation of the eyelashes on the affected side. The regional lymph nodes and parotid salivary glands should be palpated. A room with controlled lighting is ideal for examination of the globe and periocular structures, including magnification, and should be used for any animal ophthalmic exam; however, access to adjustable lighting is not always possible in equine practice. A dark blanket placed over the examiner’s and horse’s head helps create a darkened environment. The complete ophthalmic examination and derivation of a minimum ophthalmic database should be undertaken during all ophthalmic examinations with few exceptions. Components of the minimum ophthalmic database include menace response, direct and consensual pupillary light reflex, palpebral reflex, Schirmer tear test, fluorescein stain, and tonometry (Box 139-1). Tonometry must be performed with caution in any horse with a deep corneal ulcer to avoid globe perforation. Retropulsion and assessment of ocular motility are often helpful in horses with suspected orbital tumors or intraocular tumors with extrascleral extension. Retropulsion also enables the practitioner to more thoroughly examine the third eyelid (nictitans), a common site for SCC in horses. To prognosticate and plan treatment better, gentle digital orbital palpation of the orbital rim is essential. This is best accomplished with the horse sedated. Using a gloved finger lubricated with a small volume of ophthalmic ointment, insert the finger into the conjunctival fornix and palpate the entire orbital rim through the mucosa of the upper and lower fornices. Often when SCC has invaded local surrounding tissues, the orbital rim cannot be felt in areas of neoplastic infiltration.
Box 139-1 Key Components of a Complete Ophthalmic Examination for Horses with Squamous Cell Carcinoma∗
Once a complete ophthalmic examination has been performed, more advanced diagnostic imaging may be indicated, such as ocular ultrasound, skull radiographs, and computed tomography or magnetic resonance imaging. These modalities are especially helpful in horses with SCC in which evidence of bony extension is likely to alter the prognosis or surgical planning. Fine-needle aspiration of the regional lymph nodes, parotid salivary gland, or both should be performed when lymphadenopathy is detected or if there is local invasion of tumor. Definitive diagnosis of SCC should always be obtained on the basis of biopsy and histologic diagnosis. Consultation with or referral to a veterinary ophthalmologist may be helpful. Members of this specialty group can easily be located at the following URL: www.acvo.org.
Clinical Features of Ocular and Periocular Squamous Cell Carcinoma
Clinical features of SCC and its precursor lesions, which include actinic keratosis, epithelial dysplasia, chronic keratosis, and carcinoma in situ, are variable. Although SCC may arise from any location on the globe or periocular tissues, commonly affected sites include the temporal limbus, leading edge of the nictitans, and eyelid margins. Classic features of this tumor type include pink to white, raised, friable, vascularized lesions with a cobblestone- or cauliflower-like appearance (Figures 139-1 to 139-4). Necrotic tumor surfaces with a white “cake frosting” appearance from secondary bacterial infection may impart a fetid odor to the lesion.
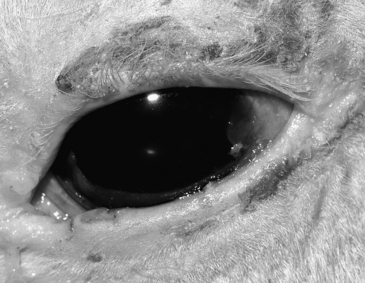

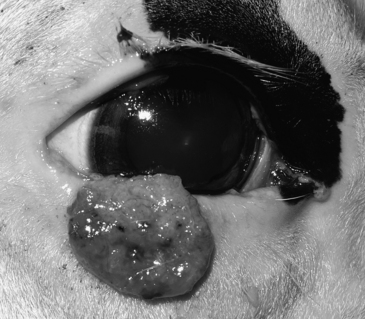
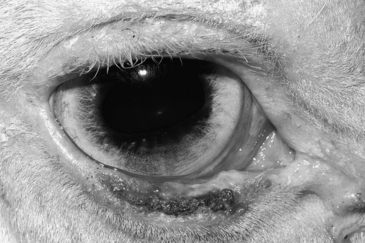
Figure 139-4 Photograph of a 9-year-old Paint mare with ulcerative squamous cell carcinoma involving the lower eyelid.
Proliferative SCC arising from the eyelid and nictitans may be pedunculated with a broad base (Figure 139-3). Ulcerated forms of this tumor typically cause erosion of the eyelid margins, medial canthus, or nictitans (Figure 139-4). Both proliferative and ulcerated forms of SCC may be present concurrently. If left untreated, local orbital invasion can ensue, resulting in substantial ocular discomfort and necessitating exenteration (Figure 139-5
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


