Chapter 19 Ocular Emergencies
The conditions discussed in this chapter are the most important disorders for which early action is necessary to prevent severe or permanent damage to the eye. Emergency treatment is outlined separately for ready clinical reference, followed by further discussion for those conditions not covered elsewhere in the text.
PROPTOSIS OF THE GLOBE
At initial presentation it is often preferable to try to salvage the globe rather than to remove it.
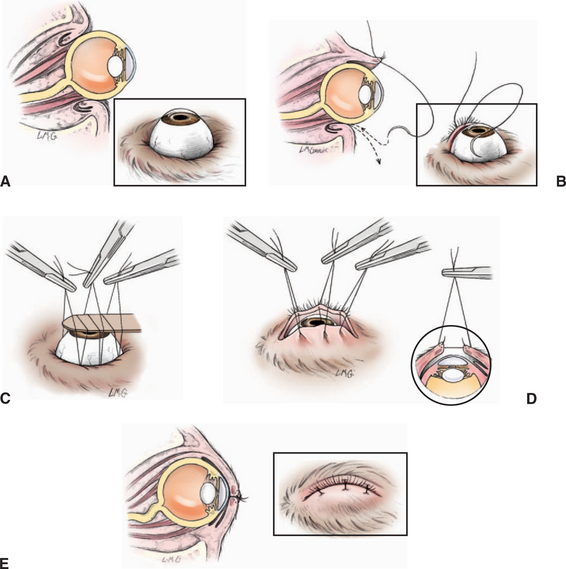
Emergency treatment for proptosis of the globe (Figure 19-1)

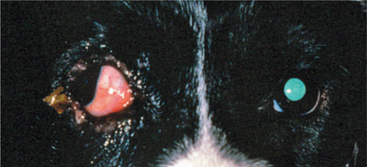
Figure 19-1 Proptosis in a young Boston terrier after a dog bite injury.
(Courtesy University of Wisconsin–Madison Veterinary Ophthalmology Service Collection.)
Prognosis
If there is any doubt as to whether the globe can be salvaged, an attempt should be made to replace it back into the orbit. The sooner the eye is replaced, the better the prognosis, both for saving the eye and for shortening the convalescent period. Unfortunately, some eyes are inevitably lost despite early and vigorous treatment. Enucleation as the initial therapy should be considered if (1) the owner is unwilling or unable to provide what may be potentially long-term postoperative care, (2) the eye has ruptured, (3) three or more extraocular muscles are torn, or (4) the eye is completely filled with blood. The following are useful prognostic indicators.
Avulsion of Extraocular Muscles
The medial and inferior (ventral) recti and inferior (ventral) oblique muscles rupture first. Because branches of the ciliary artery to the anterior segment enter the globe with the extraocular muscles, complete avulsion of three or more muscles indicates an unfavorable prognosis. In eyes with only a few of the muscles ruptured, temporary postoperative deviations (usually lateral or superolateral) of the globe occur (Figure 19-1 and 19-3). These deviations often diminish over weeks to months (up to 6 to 9 months), or the exposed conjunctiva becomes pigmented, thereby improving the cosmetic appearance of the eye. Surgical repair of the extraocular muscle tears may be indicated in select cases.
Maintenance Therapy
Keratoconjunctivitis sicca and corneal ulceration secondary to exposure are common in the postoperative period. Supplemental artificials tears or topical antibiotic ointments are often required for several weeks or longer after proptosis to lubricate the eye and prevent infection. Additionally, many severely traumatized eyes demonstrate a deep corneal vascularization that proceeds from the limbus to the center of the cornea before gradually regressing over 4 to 8 weeks. If the cornea is not ulcerated or subject to exposure, topical corticosteroids (0.1% dexamethasone or 1% prednisolone acetate) may be used every 6 to 12 hours in an effort to moderate this vascular response.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


