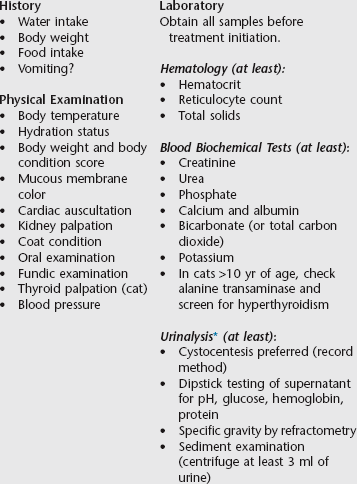
Chapter 189 The International Renal Interest Society (IRIS) has developed a staging system for chronic kidney disease (CKD) in cats and dogs that aims to improve communication about diagnosis and management of this complex syndrome. The IRIS CKD Staging system is considered a work in progress, to be reviewed and modified at least annually as additional information becomes available; the most recent version can be accessed at www.iris-kidney.com. Since its inception, the staging system has gained increasing acceptance among veterinary nephrologists and clinicians. Publications have now appeared that use this approach to report accurately staged case series, together with treatments and outcomes that improve our overall understanding of the natural history of CKD in cats and dogs and help identify better approaches to management (Cortadellas et al, 2010; Hsu et al, 2011). Consistent and accurate use of IRIS staging of CKD should help individual practitioners provide prognostic information and identify the likely consequences that require monitoring and management at the different stages of dysfunction. When faced with an animal suspected of having CKD, practitioners should adopt a logical approach to diagnosis. The recommended minimum set of data to be obtained for such patients is shown in Box 189-1. The historical and physical abnormalities that led to this suspicion should be reviewed because these findings and other evidence may highlight specific problems that warrant further investigation to determine the type of kidney disease present. This review also may indicate whether an underlying cause is likely to be identified by further investigations and whether concomitant diseases should be suspected. Box 189-1 Minimal Data Set for Patients Suspected of Having Kidney Disease *If possible, urinalysis should include estimation of the ratio of urine protein to creatinine for both cats and dogs. Laboratory evaluation should include appropriate blood biochemical tests, hematologic studies, and complete urinalysis. The results of these tests should confirm the clinical diagnosis but also may give indications of the causes and the possible presence of underlying diseases. Because kidney disease increases in prevalence as cats and dogs age, the practice of performing geriatric screening tests to detect kidney dysfunction has become more widespread. The IRIS minimum recommended geriatric screening tests for this purpose, together with a more ideal complete version, are presented in Box 189-2. The primary indicator for IRIS staging of CKD is the concentration of creatinine in plasma or serum because currently this is the most useful and readily available test of kidney function in veterinary practice. The patient must be fasting and well hydrated at the time blood is sampled. The blood creatinine concentrations used to define IRIS CKD Stages 1 to 4 shown in Table 189-1 were reached by debate and consensus based on the clinical experiences of veterinary nephrologists and data derived from longitudinal studies. As noted previously, they and other elements of staging may be modified in the future as more knowledge is gained. TABLE 189-1 IRIS CKD Staging Based on Blood Creatinine Concentration IRIS, International Renal Interest Society; CKD, chronic kidney disease. *Note that these blood creatinine concentrations apply to dogs of average size; for those of extreme size (e.g., miniature and giant breeds) these ranges may not be appropriate. Proteinuria is singled out for special attention because there is good evidence that it is a prognostic indicator in dogs and cats with CKD. For IRIS CKD substaging based on proteinuria to be used, the proteinuria must be of renal origin; therefore prerenal and postrenal causes of proteinuria have to be ruled out first. Because persistent proteinuria is considered more likely to be significant than transient proteinuria, substaging ideally requires proteinuria to be demonstrated in three or more urine samples over at least a 2-week period. It is important that urine sediment be examined microscopically on each occasion to rule out the presence of inflammation in the urinary tract (see Chapter 187). The three substages are nonproteinuric (NP), borderline proteinuric (BP), and proteinuric (P), based on the urine protein/creatinine (UP/C) ratio (determined using mass units), as shown in Table 189-2. Note that UP/C ratios classified as NP or BP may be categorized as microalbuminuric when other test methods are used. Because the significance of microalbuminuria in predicting future renal health is not understood at present, the current IRIS recommendation is to continue monitoring these patients for proteinuria using UP/C determinations. For animals found to have P or BP disease, the significance of the finding depends on the concurrent stage of CKD. Thus the P substage is more significant at Stage 3 than at Stage 1; this is because the filtered protein load presented to tubules reduces as the functioning nephron mass declines. Consequently, a given level of proteinuria has higher significance as glomerular filtration rate (GFR) declines. Note that UP/C ratios at the BP or P level can indicate tubular or glomerular dysfunction, but once the UP/C ratio exceeds 2.0 it most likely indicates a primary glomerular problem. Response to any treatment given to reduce proteinuria (see later) should be monitored at appropriate intervals using the UP/C ratio. TABLE 189-2 IRIS CKD Substaging by Urine Protein/Creatinine (UP/C) Ratio IRIS, International Renal Interest Society; CKD, chronic kidney disease.
Chronic Kidney Disease
International Renal Interest Society Staging and Management
Diagnosis of Chronic Kidney Disease
Staging Based on Blood Creatinine Concentration
Stage
Creatinine (mg/dl [µmol/L])*
Comments
At risk
As for Stage 1
History suggests the animal is at increased risk of developing CKD in the future because of a number of factors (e.g., exposure to nephrotoxic drugs, breed, high prevalence of infectious disease in the area, or old age).
1
<1.4 (125) dogs
<1.6 (140) cats
Nonazotemic. Some other renal abnormality present (e.g., inadequate urinary concentrating ability without identifiable nonrenal cause, abnormal renal palpation or renal imaging findings, proteinuria of renal origin, abnormal renal biopsy results, increasing blood creatinine concentrations in samples collected serially).
2
1.4-2 (125-180) dogs
1.6-2.8 (140-250) cats
Mild renal azotemia (lower end of the range lies within reference ranges for many laboratories, but the insensitivity of creatinine concentration as a screening test means that animals with creatinine values close to the upper reference limit often have excretory failure). Clinical signs usually mild or absent.
3
2.1-5 (181-440) dogs
2.9-5 (251-440) cats
Moderate renal azotemia. Many extrarenal clinical signs may be present.
4
>5 (>440) dogs and cats
Severe renal azotemia. Many extrarenal clinical signs usually are present.
Substaging of Chronic Kidney Disease
Proteinuria
UP/C Value*
Substage
<0.2 cats and dogs
Nonproteinuric (NP)
0.2-0.4 cats
0.2-0.5 dogs
Borderline proteinuric (BP)
>0.4 cats
>0.5 dogs
Proteinuric (P)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


International Renal Interest Society Staging and Management
Only gold members can continue reading. Log In or Register to continue
