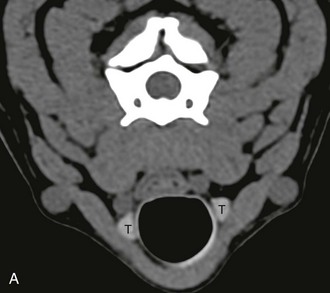
Chapter 40 The routine use of nuclear medicine in veterinary endocrinology is limited to thyroid scintigraphy. This modality is extremely useful to determine unilateral or bilateral lobe involvement, the status of the gland, the location of hyperfunctioning ectopic or accessory tissue, and distant metastases of thyroid tumors. Availability of scintigraphy is limited in veterinary medicine. Box 40-1 lists some useful imaging tips for evaluating endocrine disorders in dogs and cats. US is the primary modality for evaluation of the thyroid gland. The gland appears on US as a homogeneous, well-delineated, hyperechoic (compared with the surrounding musculature), fusiform structure. Measurements of the height (dorsoventral axis) of the thyroid gland and calculation of its volume using the formula of a rotation ellipse have the lowest variability and should be preferred in comparative and follow-up studies. On CT, the normal thyroid gland is homogeneous, ovoid or triangle-shaped, and hyperattenuating compared with the surrounding tissues (Table 40-1). The hyperattenuation is due to its natural high iodine content, which is an element with a high atomic number (53) compared with most other elements in the body (Figure 40-1, A). After intravenous injection of iodinated contrast medium, the gland shows usually diffuse enhancement. On MRI, the thyroid gland may appear heterogeneous, particularly on T2-weighted images, or homogeneous. On T1-weighted images, the thyroid gland is isointense to surrounding muscles in half of cases and shows intermediate signal intensity between fat and muscle in the other half. After contrast medium administration (gadolinium-based), the thyroid gland shows intensity between muscle and fat or is isointense to fat. On T2-weighted images, the thyroid gland shows intensity between muscle and fat. MRI is the best modality to evaluate local tissue invasion, detect cervical lymphadenopathy, and detect recurrent thyroid carcinoma after treatment. TABLE 40-1 Computed Tomography Attenuation Values of the Normal Thyroid Gland Figure 40-1 CT images of the thyroid gland. A, Precontrast CT scan of a normal adult dog shows the hyperattenuating thyroid glands (T). B, Precontrast CT study of an adult dog with a large mass (asterisk) located dorsally to the trachea and extending from the caudal part of the pharynx to the level of the sixth cervical vertebra. Both thyroid glands (arrows) were entirely visible excluding a thyroid origin. An ectopic thyroid origin is also unlikely because of the dorsal location. The mass was a paraesophageal abscess. (Courtesy Olivier Taeymans, Tufts University.) In dogs, thyroid neoplasia (mostly carcinomas, less commonly adenomas) is associated with a unilateral (66%) or bilateral (33%) mass caudal to the pharynx. Clinically detectable neoplasms usually are nonsecreting, resulting in euthyroidism throughout the course of the disease. In dogs with thyroid neoplasia, diagnostic imaging is used (1) to define the thyroid origin of the cervical mass, (2) to detect local or distant metastases, and (3) to evaluate local tissue invasion. Whatever imaging modality is used, it is sometimes difficult to document the thyroidal origin of the mass when its size severely disrupts the normal anatomy of the cervical area. Scintigraphy, CT, and to a lesser extent US may be indicated to determine whether large cervical masses arise from the thyroid gland or from other tissues. When the mass arises from tissues other than the thyroid, both thyroid lobes should be visible exhibiting a normal pattern (Figure 40-1, B). Additionally, US and CT can be used to guide a fine-needle aspiration or a core biopsy of a cervical mass.
Imaging in Diagnosis of Endocrine Disorders
Imaging Modalities in Endocrinology
Imaging the Thyroid Gland
Thyroid Gland
Canine
Feline
Precontrast attenuation (HU)
108
123
Postcontrast attenuation (HU)
169
169
Volume (mm3)
1150*
—

Canine Thyroid Neoplasia
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


