22 Hypothyroidism
CASE HISTORY
The relevant history in this case was:
CLINICAL EXAMINATION
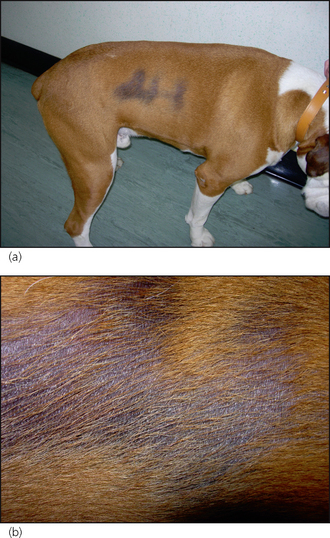
Physical and skin examinations may reveal a great variety of systemic and cutaneous symptoms that vary from case to case (Tables 22.1 and 22.2). The relevant findings in this case were:
Table 22.1 Systemic signs associated with hypothyroidism
| Common signs | Uncommon or rare signs |
|---|---|
Table 22.2 Dermatological abnormalities in canine hypothyroidism
| Common | Uncommon or rare |
|---|---|
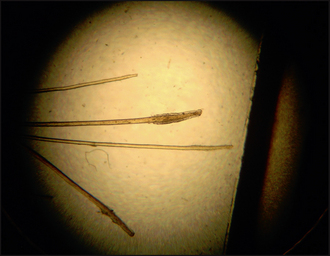
| Thin, easily epilated hair coat | Pyoderma |
| Symmetrical alopecia | Ceruminous otitis externa |
| Failure of hair growth after clipping | Demodicosis |
| Scaling | Myxoedema |
| Hyperpigmentation | Lightening of the hair coat colour |
| Comedone formation |


CASE WORK-UP
The following diagnostic tests were performed:
Blood tests for hypothyroidism
fT4ED: Basal free T4 by equilibrium dialysis (fT4ED) measures non-protein-bound circulating T4. Concentrations of fT4 will decrease in hypothyroidism, but may be maintained in early hypothyroidism, reducing the sensitivity of this test. It is expensive in comparison to TT4, but fT4 should be less affected by non-thyroidal illness than TT4 and is unaffected by the presence of AT4A. Note: some laboratories may measure free T4 using ‘analogue’ assay techniques, which is no more use than measuring TT4 alone.
In this case, the following tests were performed:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


