CHAPTER | 9 Hereditary, Congenital, and Acquired Alopecias






















Excessive Shedding


Alopecic Breeds
Treatment and Prognosis

FIGURE 9-3 Alopecic Breeds.
This Chinese Crested demonstrates the characteristic pattern of alopecia typical of this breed.


FIGURE 9-5 Alopecic Breeds.
A Sphinx cat, demonstrating the almost total alopecia typical of this breed.






FIGURE 9-11 Alopecic Breeds.
Over time, the occluded follicles form milia, which appear as white, papular lesions.

Canine Hypothyroidism
Diagnosis


























Treatment and Prognosis



FIGURE 9-15 Canine Hypothyroidism.
Mild alopecia on the bridge of the nose may be an early lesion of hypothyroidism.

FIGURE 9-16 Canine Hypothyroidism.
Alopecia and hyperpigmentation with no evidence of secondary superficial pyoderma on the trunk.






FIGURE 9-22 Canine Hypothyroidism.
Severe fading of the hair coat with partial alopecia in a hypothyroid Irish Setter.

FIGURE 9-23 Canine Hypothyroidism.
Same dog as in Figure 9-22. The extremely faded hair coat also demonstrates partial alopecia (the matting is not typical of this disease).

FIGURE 9-24 Canine Hypothyroidism.
Same dog as in Figure 9-22. Faded hair is apparent on the dorsal surface of the foot. Note the abnormal nails, which developed as a result of the metabolic effects of hypothyroidism.

FIGURE 9-25 Canine Hypothyroidism.
Same dog as in Figure 9-22. Abnormal nails developed as a result of the abnormal metabolism caused by the disease.

FIGURE 9-26 Canine Hypothyroidism.
Generalized fading caused by the lack of normal follicular cycling and hair renewal.

Canine Hyperadrenocorticism (Cushing’s disease)
Diagnosis
 ACTH stimulation test (cortisol): an exaggerated poststimulation cortisol level is highly suggestive of endogenous hyperadrenocorticism, but false-negative and false-positive results can occur. In iatrogenic cases, an inadequate response to ACTH stimulation is typical. Note: Reconstituted cosyntropin (ACTH solution) can be stored frozen at −20°C in plastic syringes for up to 6 months with no adverse effects on its bioactivity.
ACTH stimulation test (cortisol): an exaggerated poststimulation cortisol level is highly suggestive of endogenous hyperadrenocorticism, but false-negative and false-positive results can occur. In iatrogenic cases, an inadequate response to ACTH stimulation is typical. Note: Reconstituted cosyntropin (ACTH solution) can be stored frozen at −20°C in plastic syringes for up to 6 months with no adverse effects on its bioactivity.



Treatment and Prognosis


 To maintain remission after mitotane induction, mitotane PO with food 50 mg/kg administered once weekly, or 25 mg/kg twice weekly. Dogs that relapse during maintenance therapy should be reinduced with daily mitotane for 5 to 14 days or until recontrolled, then maintained with 62 to 75 mg/kg once weekly, or 31 to 37.5 mg/kg twice weekly. A great deal of patient variability occurs, requiring close monitoring.
To maintain remission after mitotane induction, mitotane PO with food 50 mg/kg administered once weekly, or 25 mg/kg twice weekly. Dogs that relapse during maintenance therapy should be reinduced with daily mitotane for 5 to 14 days or until recontrolled, then maintained with 62 to 75 mg/kg once weekly, or 31 to 37.5 mg/kg twice weekly. A great deal of patient variability occurs, requiring close monitoring.








FIGURE 9-30 Canine Hyperadrenocorticism.
Same dog as in Figure 9-29. The potbellied appearance and alopecia are apparent.

FIGURE 9-31 Canine Hyperadrenocorticism.
Same dog as in Figure 9-29. Generalized seborrhea sicca can be secondary to numerous underlying diseases but was caused by hyperadrenocorticism in this dog.


FIGURE 9-33 Canine Hyperadrenocorticism.
Close-up of the dog in Figure 9-32. As tissue wasting progressed, the scar became thin and the tissue was pulled apart.

FIGURE 9-34 Canine Hyperadrenocorticism.
The papular rash was caused by secondary superficial pyoderma.


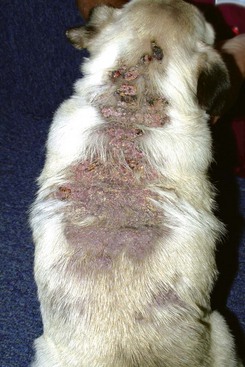
FIGURE 9-37 Canine Hyperadrenocorticism.
Extensive calcinosis cutis covering the dorsum of a dog with iatrogenic Cushing’s disease.





FIGURE 9-42 Canine Hyperadrenocorticism.
Calcinosis cutis with a severe inflammatory dermatitis in the inguinal skin fold.
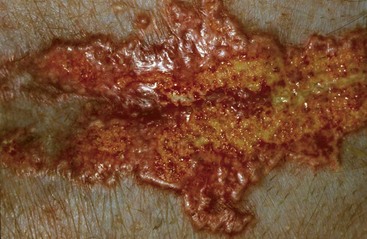
FIGURE 9-43 Canine Hyperadrenocorticism.
Close-up of the dog in Figure 9-42. The erythematous, papular plaque was caused by a combination of calcinosis cutis and secondary infection.

FIGURE 9-44 Canine Hyperadrenocorticism.
Symmetrical truncal alopecia in a dog with hyperadrenocorticism.

FIGURE 9-45 Canine Hyperadrenocorticism.
Same dog as in Figure 9-44. The sparse hair coat was bilaterally symmetrical. This dog was mildly pruritic because of a secondary superficial pyoderma.

FIGURE 9-46 Canine Hyperadrenocorticism.
Ventral alopecia with a distended abdomen in a dog with an adrenal tumor.
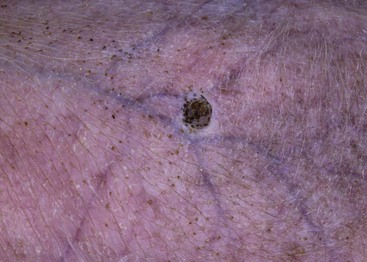
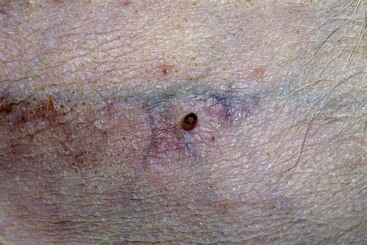
FIGURE 9-47 Canine Hyperadrenocorticism.
Phlebectasia (an erythematous papular lesion) on the abdomen of a dog with Cushing’s disease.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


