General Surgical Principles and Neutering
Anaesthesia and postoperative care are covered in Chapter 4. Endoscopy in rabbits is summarized in Table 13.1.
Table 13.1
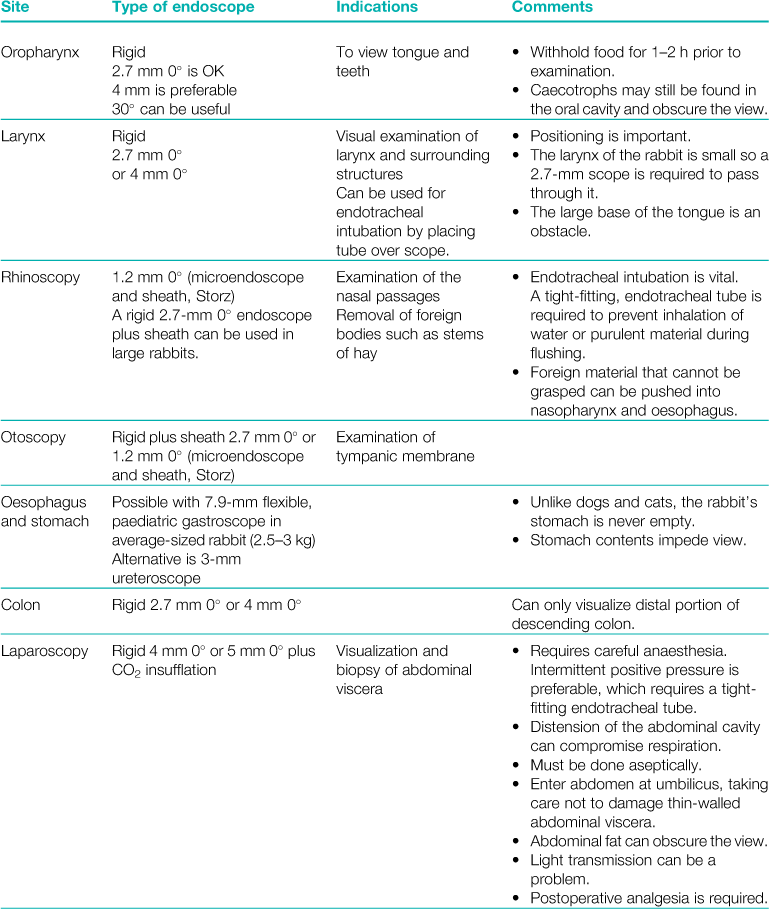

As a general rule, the largest endoscope possible should be used. Large endoscopes give a better view, with good illumination and are stronger and less liable to damage.
Rigid endoscopes are most suitable for most endoscopic procedures in rabbits. They require an irrigation sheath that is used for flushing, sucking and insufflation. A larger sheath can be used to provide an instrument channel.
General anaesthesia is required.
13.1 Skin preparation
Rabbit skin is thin and prone to injury. It contains many hair follicles with multiple shafts of fine dense hair. Removing the hair without damaging the skin or clogging the clipper blades can be difficult. A good-quality, robust set of clippers is a sound investment. Rabbit hair is so fine that it quickly becomes trapped between fine clipper blades. Running the clipper blade slowly through the fur can prevent this. Depilatory creams can be used but tend to be messy and difficult to clean off satisfactorily. The application of excessive quantities of spirit to the operation site can cause heat loss, especially in small, thin rabbits. Excessive scrubbing or iatrogenic skin damage from the clippers may cause postoperative irritation, pain and possibly self-mutilation, especially around the perineum. Chlorhexidine in spirit (Vetasept, Animalcare) is suitable for preoperative skin sterilization as it can be used as a single application and does not require skin scrubbing.
13.2 Surgical considerations
Good illumination is essential for rabbit surgery. The tissue is thin, delicate and friable in comparison with the dog or cat. Some surgeons prefer to operate using optical loupes or an operating microscope. Transparent, plastic drapes are an asset as they allow the anaesthetist to observe the respiratory movements during surgery. A set of fine surgical instruments is required. A kit has been put together especially for surgery on rabbits (Animalcare, York). It contains a selection of 5” (12.7 cm) straight and curved Criles and Halstead forceps, Martin splinter forceps, Debakey (2 mm) and Adson (1/2cm 5”) dissecting forceps, an Olsen Hegar scissor needle holder and 5” (12.7 cm) straight sharp/blunt and 4.5” (11.5 cm) Strabismus scissors. A no. 9 scalpel blade and a pair of 6” (15 cm) straight Metzenbaum scissors are also included.
The blood volume of rabbits is 55–65 mL/kg (Gillett, 1994). Up to 10% of this amount can be lost without untoward effect: above 20–25% results in hypovolaemic shock.
Rabbits are prone to the development of adhesions after surgery. The omentum in rabbits is small and it is often not possible to omentalize viscera satisfactorily. Foreign material such as talc from gloves or lint from gauze swabs can induce adhesion formation. Gentle surgical technique with minimal tissue handling is important. Fat necrosis occurs readily, especially in the broad ligament. The fat decomposes into fatty acids and glycerol that combine with ions such as sodium, potassium and calcium. It is associated with trauma.
Rabbits are used extensively as experimental models of post-surgical adhesions in humans, especially after urogenital surgery. In laboratory rabbits, it has been discovered that calcium channel blockers are effective in preventing adhesions (Steinleitner et al., 1990). Verapamil (200 μg/kg), given subcutaneously every 8 h for a total of nine doses, can be used in situations where adhesions are likely to develop. Examples include surgery on the large intestine, ruptured pyometra or abdominal abscess removal.
13.3 Suture techniques and materials
Experimental studies have indicated that the size of the suture material is more important than tissue reactivity in adhesion formation (Holtz, 1982). Therefore, the choice of fine suture material in addition to good suture technique is important for minimizing adhesion formation in rabbits. Small-gauge (3/0, 4/0 or 5/0) modern suture materials swaged on needles are satisfactory. Polydioxanone (PDS 11) or poliglecaprone (Monocryl, Ethicon) can be used for most situations, although 3/0 or 4/0 catgut is suitable to tie off blood vessels or ligaments.
13.4 Abdominal incisions
A midline approach through the linea alba is suitable for most abdominal procedures in rabbits. A good choice for repairing the incision is 4/0 polydioxanone (PDS 11) as it has high tensile strength and is degraded slowly. An alternative is 4/0 poliglecaprone (Monocryl, Ethicon). The abdominal fascia is repaired in a single layer. Studies in rabbits have shown that a double-layer abdominal closure has no advantage over a single-layer technique (Nilsson, 1981). The knots at the ends of the suture must be made with particular care if a continuous suture is used. The first throw draws the edges of the fascia together without crushing. An additional four throws are required at the start of the suture and six at the end (Bouvy and Dupré, 1997). Alternatively, a row of simple interrupted sutures can be used. Skin closure with a continuous subcuticular suture with a buried Aberdeen knot is recommended (see Figures 13.1 and 13.2) (Flecknell, 1998). Additional skin sutures or tissue adhesive can be used, if necessary. Owners appreciate skin sutures and worry that the patient has removed them if they cannot be seen. It is important that the abdominal incision is repaired securely and without tension on the sutures. Tight sutures and ischaemia of the peritoneum increase the risk of abdominal adhesions (Niles and Williams, 1999). If the suture line is comfortable, most rabbits will leave the incision alone, although some will remove the skin sutures. If the subcuticular suture is secure, this is not important.
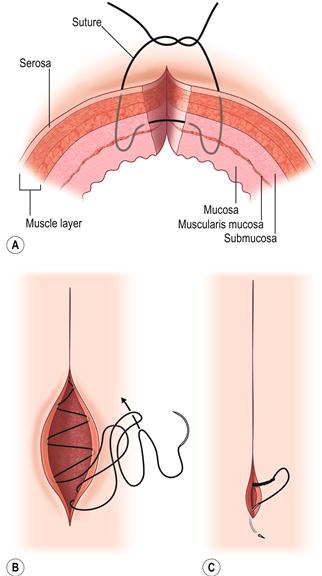
Figure 13.1 Recommended suture patterns.(A) Modified Gambee suture pattern for edge-to-edge intestinal repair.
The submucosal layer is important during intestinal healing due to its abundance of collagen. During repair, it is essential to pass sutures through the submucosal layer and to bring it and the wound edges into direct apposition without crushing the tissue or everting the mucosa. Single-layer enterotomy closures are preferable because double-layer closures reduce the lumen diameter. Classic inverting sutures can induce stenosis, which is a major problem in rabbits that have a narrow intestinal lumen. Fine (5/0), absorbable, monofilament suture material such as poliglecaprone (Monocryl, Ethicon) or polydioxanone (PDS II, Ethicon) are suitable for the closure of intestinal incisions. A modified Gambee suture, using single interrupted sutures 2–3 mm apart and 2–3 mm from the cut edge, is satisfactory. With correct instrumentation, this suture pattern is surprisingly easy.(B) Subcuticular skin closure using an Aberdeen knot.
Skin sutures can easily be removed by rabbits although, if the suture line is comfortable, most rabbits will leave a surgical incision alone. Elizabethan collars are unsatisfactory and stressful to rabbits and are not an alternative to good surgical technique. It is important that surgical incisions are repaired securely and without tension on the sutures. Skin closure with a continuous subcuticular suture with a buried Aberdeen knot is recommended (Flecknell, 1998). This method leaves no visible skin sutures for the rabbit to remove. Fine, absorbable, monofilament suture material such as poliglecaprone (4/0 Monocryl, Ethicon) or polydioxanone (4/0 PDS II, Ethicon) are suitable for subcuticular suturing.(C) Finishing the Aberdeen knot.
This is done by tunnelling the free end under the skin for a short distance and pulling the knot end tight subcutaneously before cutting the free end of the suture as it exits the skin surface.





Figure 13.2 Subcuticular skin closure using an Aberdeen knot.
(A) The subcuticular suture is placed normally. Once completed, a loop of suture material is created by taking a bite of tissue along the suture line with the needle, pulling the suture material through but not tightening the stitch completely.
(B) The free end of the suture material is then looped through the original loop, making a second loop.
(C) The first loop or throw is then tightened by pulling firmly on the end of the suture material nearest the original loop.
(D) This process is repeated several times to create a knot.
(E) For the final throw the free end of the suture material is pulled through the loop, and the loop is pulled tight.
(F) The free end of the suture is then secured by using the needle to pull the suture material under the skin, exiting the skin a short distance from the wound, meaning that there is not a free suture end left in the wound. The end of the suture material is pulled through the skin and cut off at the skin level.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


